Fed is Best Foundation receives stories from mothers who have been led to harm their infants in the pursuit of increasing exclusive breastfeeding rates. Learn about the dangers of insufficient feeding in breastfed infants caused by Baby-Friendly Hospital Initiative.
Did you know combo-feeding is the most common way to feed babies worldwide? In the US, 75% of babies and 59% globally receive infant formula during the first year of life, yet it is often overlooked in new parents’ infant feeding education and support. Given these significant statistics, parents shouldn’t have to navigate alone or rely on friends, family, and social media for potentially inaccurate information that could compromise the health of infants or breastfeeding itself.Continue reading →
Good information isn’t always enough to overcome bad systems.
By Sarah Christopherson
I wrote this article in late 2018, a few months after giving birth to my daughter. My experience at my “Baby Friendly†hospital was traumatic and it was painful to relive, but I felt like I could help other new parents by telling my story, and it seemed like a good match for the work I was doing professionally to dismantle coercive systems that deprive women of their autonomy.
At the time, I was the policy advocacy director for a national non-profit focused on empowering women as they navigate healthcare in the US. My article was printed in our organizational newsletter in early 2019 and published on our website.
It was shared by Fed Is Best, which also interviewed me. From time to time, I would send the link to expecting parents, not to scare them, but to empower them to stand up for themselves when they sensed that something wasn’t right. It helped me to help others. And telling my story made a difference.
A friend who gave birth in the same hospital texted me, “Your article helped me so much when I was having trouble breastfeeding. I look at the pictures of [my son’s] early days and think about how it would have gotten worse if I hadn’t talked to you and others. I started supplementing with formula early AND I signed that dumb form without blinking. The post-partum period exhausts you so that normal problems you would easily solve seem so much harder… and then you’re dealing with some of the most consequential decisions you’ve ever had to make. It was the things I’d already thought through a bit—like the stuff in your piece—that I was prepared to tackle.â€
Eventually my non-profit changed leadership and I moved into a different policy field. My infant turned into a happy, healthy, precocious, and articulate 6-year-old bouncing ball of energy. And that’s where I thought things ended.
Until last week, when I discovered that without my knowledge or permission, my former organization had rewritten my article in January. They’d kept my name, my story, and the picture my husband took of me in a hospital gown holding my infant daughter on the day she was born. But they’d stripped out paragraph after paragraph that cautioned against breastfeeding coercion.Continue reading →
My breastfeeding journey was not at all what I envisioned for my little one and me. When I was pregnant with my firstborn, I heard stories from my mom that she never used a bottle with my brother and me. When I researched breastfeeding, parents were told how wonderful and natural it is. I believed breastfeeding would come naturally.
The day my son was born was a whirlwind. I had to have a c-section due to complications, but we were so excited to meet him. The first few days, I tried to get him to latch on, and he would stay for a little while and then unlatch. I felt uneasy that he wasn’t getting enough colostrum, but the medical staff told me I was doing great. My husband and I were so focused on getting breastfeeding down that I forgot to get pictures of me and my little one. My focus was getting him fed the right way. Sometimes, nursing hurt so much that I would dread it when it was time for feeding. The on-site lactation consultant came the day after the c-section. She was with me for an hour and told me everything was wonderful! After she left, my baby would cry, and I knew something wasn’t right. My husband and I decided it was time to ask for formula. When we asked, the nurse kept asking us if we were sure. As first-time parents, we questioned if we were doing the right thing.
I was so tired and needed rest that my husband fed my little one formula. A nurse came in and said, “Dad! Don’t! Breastfeeding is the way! Don’t do that to your little one. Your wife is doing great.” She grabbed the formula from my husband’s hands and stashed it in a cabinet. My husband and I looked at each other in shock, and I tried to breastfeed again.
We were discharged on a Friday, and over the weekend, my son cried a lot, and I thought he might be a fussy baby. On Monday morning, we saw that my son had orange urine in his diaper. I lost it. I remember holding him and crying, blaming myself. We went to the doctor’s office and were told that he was dehydrated. He also lost a lot of weight, more than he should have, and my doctor suggested it was time to supplement my baby with formula.
After that, I cried for hours, and I could not get over the guilt. I kept thinking: “Why didn’t I know he was hungry or not getting enough? How could I have let my baby starve?” The guilt stayed with me for months.
This event was what I believe was the catalyst for my PPD/PPA.
After that, I became obsessed with feeding my son. I would write down how many ounces of formula or breastmilk he had and at what times. I no longer breastfed, but I pumped, so I knew exactly how many ounces he was consuming. Even when he was a few months older, I would still wake him up to feed him because I thought he would become dehydrated again. I hated when my little one would cry because it would be a reminder of the terrible weekend of his life, and I would break down, and I would cry. I spent so much of the first year of his life blaming and shaming myself for unintentional starvation.
My husband and I hope to have another little one, and I know what I would do differently. I feel guilty that my little one had a rough start on his feeding journey, but I try to remember that as he was learning, I was also learning.
I can’t tell you how much I appreciate Fed is Best Foundation and their work. I honestly don’t know what would have happened to me without finding your community. I got so emotional writing my story. Thank you for being there for mothers and babies.
Frequent breastfeeding and cluster feeding are often used interchangeably, creating confusion for parents. This educational blog will help parents clarify the differences between the two.
What are the differences between frequent breastfeeding and cluster feeding before lactogenesis II for newborns?
Frequent Feeding-Newborn babies feed frequently (every 2-3 hours) beforelactogenesis II, the onset of copious milk production. Frequent feeding is expected and normal.
Cluster Feeding-Cluster feeding occurs after the arrival of lactogenesis II and is defined as a series of short feeding sessions lasting 2-3 hours daily.
As a result of my traumatizing breastfeeding experience, I became an IBCLC. My goal as an RN and IBCLC is to help moms reach their feeding goals in a safe and evidence-based way and, most importantly, to ensure that babies are fed, not forced to go hungry, and to listen and believe moms when they say they are notmaking enough milk! After all, the number 1 rule in lactation is to feed the baby, but that rule no longer applies. The rule is to breastfeed exclusively, at all costs. That was the price my baby had to pay, and I am determined to change that.
I was just beginning my career as a labor and delivery nurse when I became pregnant with my first child. According to our standard breastfeeding policies, all our patients were encouraged to breastfeed. It was common for patients to complain that they didn’t have enough milk, but we were taught this was “rare” as babies have small stomachs and need little colostrum. Because of this, I assured my patients that everything was fine.
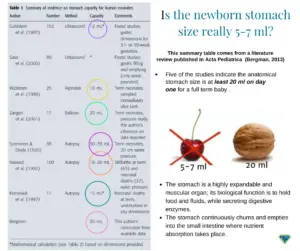
There is a myth regarding a newborn’s stomach size that perpetuates the underfeeding of EBF babies, and now it is beginning to infiltrate formula-fed babies as well. The myth is found in every hospital and is not supported by current research. According to seven research articles, the stomach size of a term 7-pound baby ranges between 20 and 35 ml.
Another myth is that colostrum is all your baby needs. Note: One teaspoon of colostrum contains three calories. Feeding a newborn baby drops of colostrum is never enough for adequate feeding and fluids.
There is also a myth that low milk supply is rare.
Scientific Studies SHOW THAT DELAYED ONSET OF LACTOGENESIS II (DOLII), LACTATION DYSFUNCTION, AND LOW MILK SUPPLY (LMS) ARE COMMON.
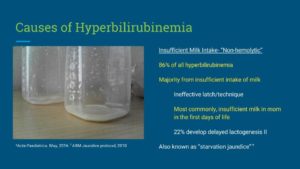
After my first baby was born, I immediately began breastfeeding her, and everything seemed to be going well with latching and nursing, but she cried a lot, which was unsettling to me as I couldn’t comfort her. However, excessive crying was considered normal. (Note: Excessive crying is not normal) Gradually, my baby developed excessive jaundice, and the neonatologist was so concerned he recommended supplementing her with formula after nursing before we could be discharged. I tried to hand express, and all I could get was the tiniest clear drop, but the IBCLC said I probably didn’t respond to hand expression and told me I didn’t need to supplement because my baby’s bilirubin level wasn’t “too high.” Sadly, I followed the advice of the IBCLC. (Note: The IBCLC violated her Code of Professional Conduct and Scope of Practice, putting this baby in unsafe conditions without adequate nutrition and fluids and increasing bilirubin levels.)
That night, my baby did not sleep at all because she was crying. As I slept, my husband tried latching her onto my breasts as I was exhausted and falling asleep. In the morning, she was re-examined, and her bilirubin levels got worse, and she also lost a whopping 10 ounces! I was told by the neonatologist that I needed to supplement urgently.
With terror in my heart, I trembled, and I began supplementing right away. My baby finally stopped crying and slept for the first time.
I nursed and supplemented her every 2 hours because she was so hungry. However, another IBCLC and the breastfeeding support group I was in told me that supplementing my baby would hurt my supply, so I slowly eased her off the formula and began EBF again at one month old. (Note: supplementing does not decrease milk supply if adequate breast stimulation and milk removal are provided with every supplemental feeding.)
Even though I was finally exclusively breastfeeding, my baby would nurse every 15 minutes, and I would have maybe one 15-minute break all day when my husband took care of her. She would cry the whole time. Whenever she fed, I told myself it was “cluster feeding.” Her continuous feeding was good for my supply; I should keep it up.
Cluster feeding is another myth parents are taught when babies feed non-stop in the hospital. Find out what “cluster-feeding” really is here: cluster-feeding
I went to see another IBCLC, and she did a weighted feed. After feeding her, the weight didn’t change at all. The IBCLC said a mistake must have occurred, “that never happens.” She suggested I come back after another weighted feeding when my breasts were painfully full. At this weighted feeding, my baby had only gained one ounce, but I was only encouraged to continue exclusive breastfeeding because her weight was slowly going up. (Note: The IBCLC violated the Code of Professional Conduct and scope of practice. The baby was placed in unsafe conditions because of inadequate feeding. The baby should have been supplemented, and a feeding plan should have been implemented to improve milk supply while supplementing. Her pediatrician should have been notified; follow-up lactation appointments to monitor weight gain were essential.
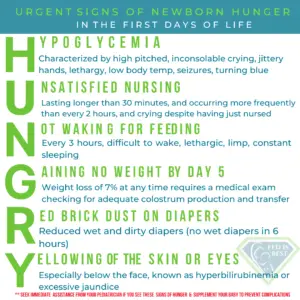
At nine weeks old, despite me constantly nursing her, her weight percentile dropped from the 76th percentile at birth to 7th. She had gone ten days without pooping; she even had a few brick dust diapers during the month of exclusive breastfeeding. At this point, I was at my breaking point. Both my baby and I were not thriving. I vividly remember reading the signs of HUNGRY on the Fed Is Best website in the middle of the night. I burst into tears knowing my baby had some of the symptoms and realized she was hungry!
There was no way to describe the guilt I felt. The truth is no mother can believe she wasn’t giving her baby enough milk when she was doing the “right” thing by exclusively breastfeeding. The result was that I had to suffer through the depths of the worst mom guilt hell.
The fact that she ate all the time was not normal. Still, many breastfeeding support groups said it was all normal (cluster feeding, baby can go two weeks without pooping, percentile charts are not accurate for breastfed babies, and some babies are just smaller, etc.).
These breastfeeding support groups are harming babies every day, and I shudder to think about how many babies are suffering from hunger or worse.
My pediatrician recommended I begin supplementing with formula again, and I finally decided I needed my baby to be happy and healthy. I began following the Fed’s Best Supplementation Guide and supplemented with 15cc at a time after breastfeeding both sides and using a slow-flow nipple when supplementing her.She gained five ozs in two days, was finally content and happy, and began sleeping better. Her weight gain percentiles began CLIMBING rapidly, and I was so relieved.
I am here to tell you it’s possible to successfully combo-feed your baby; I successfully combo-fed my baby until she was a year old, with 1/3 of the milk from my breasts, and the rest was life-saving infant formula.
She has grown into a healthy, intelligent, beautiful girl in four years. I have since had two more children, and I have combined breastmilk with formula from the start.I still sometimes feel a pit in my stomach, wondering what would happen if I continued exclusively breastfeeding. I am so grateful to Fed is Best Foundation for helping me see the evidence that my baby was hungry.
Sarah F., RN, IBCLC
Dec 12, 2018–The aim of this Scope of Practice isto protect the public by promoting that all IBCLC certificants provide safe, competent and evidence-based care
Breaks down everything you need to know about the dangers of insufficient feeding in newborns and infants
Reveals myths around colostrum and the expectation that mothers will “naturally” produce all the milk their baby needs if they follow current guidelines
Provides detailed guidance for how to tell if your baby is getting enough to eat, particularly in those crucial first few days of life
Shares supplementation strategies that protect and encourage continued breastfeeding
Details what parents need to know about combination feeding, with sample schedules
Let Fed Is Best help you find the feeding method that’s right for you and your baby–whether that’s exclusive breastfeeding, exclusive formula feeding, or anything in between.
How can you help?
Send us your stories.Share with us your successes, your struggles, and everything in between. Every story saves another child from experiencing the same and teaches another mom how to feed her baby safely. Every voice contributes to change.