The phraseology of Fed is Best is frequently misinterpreted, and we want to clarify what it means to our readers.Nutritionally speaking, “fed” refers to the absorptive state or the first stage of nutrition, in which a baby receives adequate nutrition to maintain optimal bodily functions and achieve healthy growth and development.
Fed is best means a baby can achieve this fully fed state required to thrive from two clinically-approved sources of nutrition. One is human milk, and the other is infant formula.
Source: Science Simplified, May 13, 2020,Biology/Physiology,Video focused on details of Fed State of Metabolism.
The Fed is Best Foundation works to identify critical gaps in current breastfeeding protocols, guidelines, and education programs. We provide families and health professionals with the most up-to-date scientific research, education, and resources to practice safe infant feeding with breast milk, formula, or a combination of both. To be fully informed, parents must be taught about the risks of insufficient breast milk intake while supporting exclusive breastfeeding in order to eliminate preventable hospitalizations for insufficient feeding complications. Finally, we strive to eliminate infant feeding shaming while prioritizing perinatal mental health.
We will be answering 20 questions that we have received, and this blog is Part 1.
Questions:
1. Why do you spend so much time on the risks of exclusive breastfeeding and so little on the benefits?
We promote safe breastfeeding because no other health organization informs parents about the risks and how easy they are to prevent. As part of this mission, we wantlactating parents who choose to exclusively breastfeed to be successful in their long-term goals while ensuring the safety and long-term health and development of their infants.
For parents who wish to avoid formula use, we believe that donor milk should be made available in hospitals if supplementation is needed so that they can meet their exclusive breast milk feeding goals. But for mothers who wish to use formula supplementation in order to avoid donor milk, their wishes should be respected as well.
Formula milk has a healthy place in infant feeding and saves lives too, particularly for infants whose mothers cannot produce enough milk. We believe that characterizing properly-prepared formula as substandard or even dangerous, as has been done by many exclusive breastfeeding advocacy groups, is irresponsible and puts infants and mothers’ lives at risk. Furthermore, it is untruthful and emotionally abusive to families who use it.
We feel that hospital infant formula “informed consent” forms that deliberately characterize supplemental formula as harmful provide inaccurate information and can lead parents to avoid formula supplementation that may ultimately prevent serious outcomes. Given that the multiple diseases commonly listed have not been studied in cases of short-term formula supplementation in properly controlled trials, there is no proven causal relationship between judicious formula supplementation and these negative health outcomes.
A consent form mothers are required to sign before feeding their babies formula.
Example of text scripting given to nurses to respond to parents who are asking to feed their babies formula, using pacifiers or the nursery.
Example of text scripting given to nurses for parents who are asking for formula, pacifiers or the nursery.
We also feel that the message that exclusive breastfeeding is best for all lactating parents and infants is not only inaccurate given how common it is to be unable to sustain breastfeeding even with maximal lactation support, but it also leads to thousands of preventable hospital admissions every year in the U.S. alone. As health care professionals we take an oath to do no harm and readmitting a previously healthy newborn who has become critically ill because they did not receive enough breast milk as a result of our counseling is a violation of that oath and should be a “never event.” Unfortunately, it has become a routine, even expected outcome of exclusive breastfeeding promotion that occurs in every hospital that uses the Baby-Friendly protocol.
According to the National Quality Forum (NQF), “never events” are errors in medical care that are clearly identifiable, preventable, and serious in their consequences for patients, and that indicate a real problem in the safety and credibility of a healthcare facility.
Breastfeeding Benefits
2. How can a doctor and nurse IBCLC support the idea that formula and breast milk are equal? Do you think formula is as good as breast milk?
Our message has always been that breast milk has health benefits for babies, and breastfeeding also has health benefits for mothers. When we study breastfeeding vs. formula-feeding, there appear to be advantages to breastfeeding on average. One advantage is the reduction of gastrointestinal and respiratory infections which may be related to the presence of infection-fighting antibodies or other immune factors in breast milk that is not present in formula.
There hasnever been a time that we said formula milk and breast milk are the same. We want to make this very clear as our message has been co-opted by others in order to discredit the Fed is Best Foundation’s mission.
The health benefits of breastfeeding for both mother and baby are well documented in the scientific literature and include:
Reductions in necrotizing enterocolitis in premature infants
A small but measurable reduction in SIDS and childhood leukemia
However, the scientific data has also shown, when we account for maternal income, education and even maternal intention to breastfeed, those advantages are not so solid. When comparing breastfed versus formula-fed siblings, the differences in health outcomes and intelligence are even less. Furthermore, the studies are unable to account for the effects of breast milk supply on infant health outcomes, which vary widely. Feeding complications in breastfed infants who do not get timely and adequate supplementation also have negative health consequences, which are not accounted for in those studies, but may ultimately affect outcomes in babies are categorized as “formula-fed.”
For individual mother-baby dyads for whom breast milk is insufficient, where breastfeeding causes excessive maternal sleep deprivation and postpartum depression or otherwise fails to allow the mother and baby to thrive physically and emotionally, there are clear harms to promoting exclusive breastfeeding and characterizing formula as substandard or harmful. For those mothers and babies, partial or exclusive formula-feeding may provide the best health outcomes over breastfeeding. For a smaller portion of mother-infant dyads, breastfeeding is contraindicated, like for galactosemia.
The promotion of exclusive breastfeeding has taken an irresponsible detour by demonizing formula milk in the hopes of encouraging mothers to exclusively breastfeed when for up to 15% of the population, it is not only impossible, it is unsafe. Formula milk has been depicted as a dangerous form of nutrition for babies, which is absolutely false. The intent is to shame and guilt parents for using it. Such characterization of formula as harmful and substandard puts infant lives at risk as mothers with insufficient milk have and will sometimes unwittingly starved their infants in order to meet the socially expected standard of exclusive breastfeeding, particularly if they are not informed of the harmful consequences like impaired brain development and disability.
The image above is an example of a bullying tactic mothers are subjected to.
Laura: At first, I felt like a total failure and could not understand why my breasts would not do what they were supposed to. I would sob as I fed her. But over time I saw how much she was thriving and I started to forgive myself. I truly believe supplementing and then EFF saved me from hurting myself and allowed me finally to love my baby.
When a breastfeeding mother does not make enough breast milk, they are taught to avoid formula supplementation, while not being taught the signs and consequences of insufficient feeding. They will follow their health professionals’ advice even if their child exhibits persistent hunger until it becomes blatantly obvious that their child is critically ill. Formula milk is a nutritious food for babies and it does not need to be denigrated to encourage mothers to breastfeed. In a world where breastfeeding insufficiency is common, families need to be told how to recognize insufficient feeding and how to properly prepare formula when supplementation is needed. Such information should also be respectfully provided to families who make the informed-decision to formula-feed without judgment or harassment from health professionals.
We acknowledge and condemn the scandalous actions of Nestle corporation in the 1970s where formula was aggressively marketed to mothers in developing nations and ultimately led to the death of millions of babies from malnutrition and gastrointestinal illness from contaminated and diluted milk. It has created a very negative bias among some lactation professionals against formula itself. Let’s start separating the product, which was developed by doctors and is tightly regulated by the FDA, from the ethical violations of its manufacturer. We cannot let history be repeated by allowing aggressive marketing of the exclusive breastfeeding policy to harm millions of babies in the form of insufficient feeding complications, injuries, and deaths. Infant formula has saved millions of lives. Ethical and safe support of breastfeeding and formula-feeding are needed in order to achieve optimal health and development for all infants across the globe.
We will continue to support and protect breastfeeding without denigrating formula use because it’s the ethical thing to do. We believe that being respectful of formula-feeding families and of formula itself is not anti-breastfeeding, it is responsible, inclusive, and pro-safe infant feeding for all infants.
3. Why do you promote formula instead of donor milk?
We absolutely support screened banked donor milk and think it should be widely available for mothers who want to use it. The reality though is that it is not currently available to most term babies due to its limited availability and the need to prioritize its use in premature babies. While banked donor milk for short-term supplementation may be feasible and covered by health insurance, long-term supplementation with banked donor milk is financially not feasible for most families.Casual breastmilk donation and sharing, especially obtained from people through the internet, is particularly unsafe as it can carry transmittable infections and be contaminated with bacteria from inappropriate handling and storage. While we don’t shame mothers who use it, as licensed health care professionals, we follow the AAP and the CDC recommendations on casual milk sharing.
Ultimately, we need to work with the current situation that mothers are in, and most of the time safe donor milk is not feasible. Our top priority is to make sure babies are sufficiently fed.
4. How do you respond to concerns about “scaring new mothers” so they don’t even try to breastfeed because of the stories you write about?
We know our blog stories are very difficult to hear. Our intention is not to scare anyone, but to raise awareness on the risk factors and signs of feeding complications and by giving accurate information to mothers and health professionals. All parents are informed by their health professionals about other difficult but necessary parenting topics such as car seat safety, safe sleep practices, and even shaken baby syndrome to help prevent injury or death.But they are not told about the risks and serious consequences of inadequate breast milk intake to their babies and how to prevent complications.
We provide parents an actionable breastfeeding plan that allows them to make informed decisions in cases of insufficient or delayed copious milk production while protecting their right to successfully breastfeed. Parents commonly give us positive feedback on our breastfeeding plan and are thrilled when they are able to meet their breastfeeding goals safely and without the tears and trauma (for both mom and baby) that some experienced during their first attempt. Many moms report succeeding in sustaining a breastfeeding relationship that they could not while following the rigid rules of the WHO Ten Steps.
We oppose inaccurate ”fear-mongering” campaigns by lactation professionals, which began in 1996 when lactation consultant Diane Wiessinger wrote an article that was published in the Journal Of Human Lactation called “Watch Your Language! ”
She wrote:
“When we fail to describe the hazards of artificial feeding, we deprive mothers of crucial decision-making information. The mother having difficulty with breastfeeding may not seek help just to achieve a “special bonus”; but she may clamor for help if she knows how much she and her baby stand to lose. She is less likely to use artificial baby milk just ‘to get him used to a bottle’ if she knows that the contents of that bottle cause harm.”
Wiessinger’s goal was to inform parents of the “risks of formula feeding,” and it worked.
Every single parent who contacted us told us they were terrified to supplement their hungry babies, even when medically necessary, because of this message! Some parents refused to supplement, opting for IV glucose, unscreened and untested breast milk, or homemade formula when human milk was unavailable.
Dr. Alison Steube reinforced Wiessinger’s message in 2009 when she wrote a blog for The Academy of Breastfeeding Medicine:
“We need to talk about the “risks of formula feeding” so that we hold policy-makers and health care providers accountable. The “Booby traps” are more than a clever pun: they are a public health problem that’s undermining the health of women and their children.”
“I’ve also thought about the risks of risk vs. benefit language when talking with health professionals. Shouldn’t we use breastfeeding as the normative standard in that context? Here, again, I’ve not found a study. It would be ideal to compare a health provider’s motivation to engage with patients after hearing a talk on the “risks of formula” vs the “benefits of breastfeeding.” However, my experience is that in every audience, there are parents, and there are friends and relatives of parents. For many, the topic of infant feeding stirs deep emotions. And when we frame the conversation about “risks of formula,” there’s a real risk that we will trigger negative emotions that will cause those in the audience to shut down, such that they will not be able to hear the evidence-based, clinically applicable messages that could enable their patients to achieve their own infant feeding goals [our emphasis].”
In 2010, Marsha Walker, RN, IBCLC stoked the fear in her article Just One Bottle which was also intended to persuade parents to avoid formula citing risks of formula that are mostly speculative. But the message of this campaign continues to be taught to parents daily.
Our ultimate goal should be the goal of every health care professional: to prevent feeding complications and ensure infant safety by informing parents of both the risks and benefits of all their infant feeding choices in an ethical and unbiased fashion. This includes teaching parents that supplementation to prevent hunger and feeding complications can be achieved while ensuring sufficient stimulation to preserve and maximize the breastfeeding relationship.
5. How can you prove you aren’t connected to the formula industry?
We have responded to these accusations by sharing our tax returns as proof. All of the money that we spent to launch our Foundation was from our own personal bank accounts and we continue to use our own money for expenses. We receive modest donations from families and health professionals who believe in the Fed is Best mission and/or have witnessed the harms of aggressive pursuit of exclusive breastfeeding personally and/or professionally. We have also been compensated for assisting in medico-legal cases of infants who have suffered brain injuries from insufficient breastfeeding complications, all the proceeds from which are donated back to the Fed is Best Foundation.
The Fed is Best Foundation, without exception, has not and will not accept any donations from formula- or breastfeeding-affiliated companies or organizations to avoid conflicts of interest. In order to maintain the integrity of the Fed is Best campaign, we routinely monitor for unauthorized use of the “Fed is Best” trademark and send cease-and-desist letters to companies who try to use it to promote their infant feeding products or services.
Ultimately, our organization is an all-volunteer, grassroots organization that includes 1200 parent advocates and over 200 nurses, doctors and allied health professionals who believe in the Fed is Best mission. We are rapidly growing and currently have over 720,000 supporters because of our inclusive and responsible message and because of the passionate support of our volunteer supporters.
THANK YOU FOR YOUR INTEREST IN THE FED IS BEST FOUNDATION!
Our mission statement is:
The Fed is Best Foundation works to identify critical gaps in current breastfeeding protocols, guidelines, and education programs. We provide families and health professionals with the most up-to-date scientific research, education, and resources to practice safe infant feeding with breast milk, formula, or a combination of both. To be fully informed, parents must be taught about the risks of insufficient breast milk intake while supporting exclusive breastfeeding in order to eliminate preventable hospitalizations for insufficient feeding complications. Finally, we strive to eliminate infant feeding shaming while prioritizing perinatal mental health.
HOW YOU CAN SUPPORT FED IS BEST
There are many ways you can support the mission of the Fed is Best Foundation. Please consider contributing in the following ways:
Join us in any of the Fed is Best volunteer and advocacy, groups. We currently have– Health Care Professional Advocacy Group, Advocacy Group, Research Group, Volunteer Group, Editing Group, Social Media Group, Legal Group, Marketing Group, Maternal Mental Health Advocacy Group, Private Infant Feeding Support Group, Global Advocacy Group, and Fundraising Group. Please send an email to Jody@fedisbest.org– if you are interested in joining any of our volunteer groups. For our health professional advocacy group, join us here.
If you need infant feeding and parenting support, we have a support group– Join us here.
Make a donation to the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign theFed is Best Petition at Change.org today, and share it with others.
Share the stories and the message of theFed is Best Foundation through word-of-mouth, by posting on your social media page and by sending our FREE infant feeding educational resources to expectant moms that you know. Share the Fed is Best campaign letterwith everyone you know.
Print out ourletter to obstetric providers and mail them to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
Write your local elected officials about what is happening to newborn babies in hospitals and ask for legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
Send us your stories. Share with us your successes, your struggles and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
Send us messages of support. We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
Shop at Amazon Smileand Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!
6. Does the FIBF believe all exclusively breastfed babies need supplementation before the onset of mature milk?
No, and we never have.
As health care providers, we have an ethical and moral obligation to fully inform mothers of both the benefits and risks of exclusive breastfeeding when promoting exclusive breastfeeding. The high rates of delayed onset of lactogenesis II, as well as conditions that cause a poor transfer of breast milk, carry serious risks to exclusively breastfed newborns, as they depend ondaily increases in calories and fluids until mature milk arrives on day three.
The current research tells us the actual rates of adequate breast milk production are unknown and the current estimates for lactation disruption range from 12-15% or one in eight mothers. We are learning that mothers are experiencing delayed lactogenesis II (onset of full milk supply greater than 72 hours post-birth) commonly, for complex biological and other unknown reasons. However, the fact that something is common does not mean it is normal or ideal.
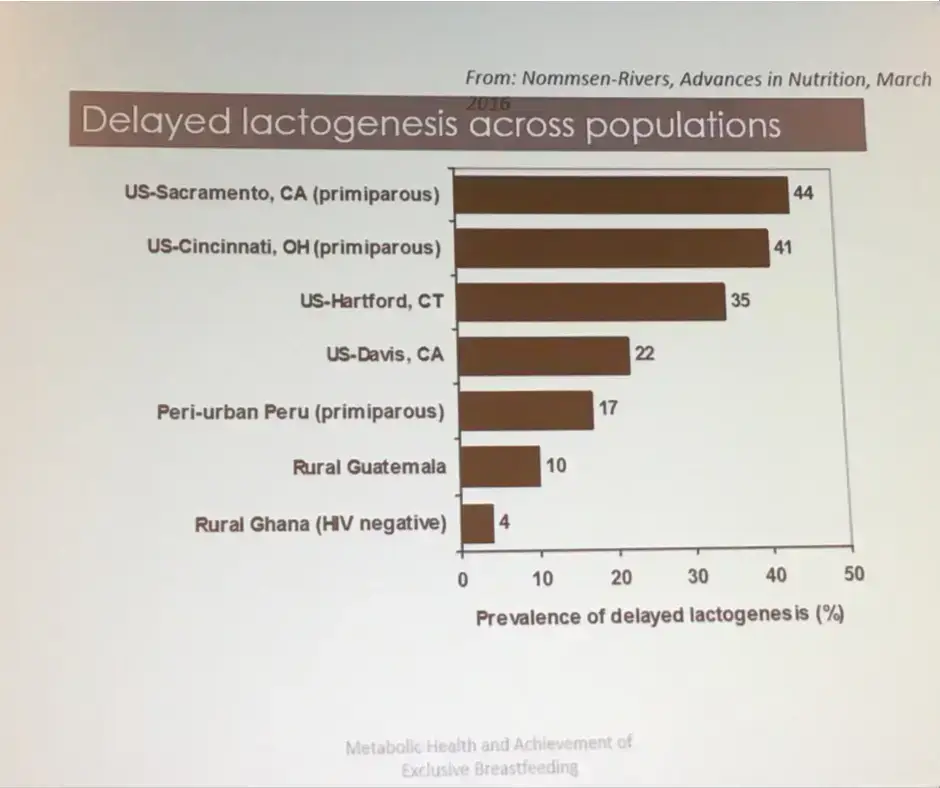
Nommsen-Rivers, Percent of mothers experiencing delayed copious milk production. Presented at 2017 ABM conference
The scientific studies show that delayed onset of lactogenesis II (DOLII), lactation dysfunction and low milk supply (LMS) are common.
Twenty-two percent of mothers experience delayed onset of milk production, which increases the risk of excessive weight loss (>10%) in their newborns seven-fold (Dewey et al., 2003). Delayed onset of lactogenesis II (DOLII) was most common among first-time mothers, mothers with high BMI, and other factors that increased the risk of ineffective breastfeeding.
Delayed onset of lactogenesis II also occurred commonly outside of the U.S. as found in this study from a Brazilian Baby-Friendly Hospital showing it occurred to 19% or almost 1 in 5 mothers. (de Oliveria Rocha et al., 2019)
Another study of first-time mothers showed that an astounding 44% experienced delayed onset of lactogenesis II. (Nommsen-Rivers, et al. 2010). The primary risk factors for DOLII were:
maternal age ≥30 years old
body mass index in the overweight or obese range
birth weight >3600 g
absence of nipple discomfort between 0–3 d postpartum
infant failing to “breastfeed well” ≥2 times in the first 24 h
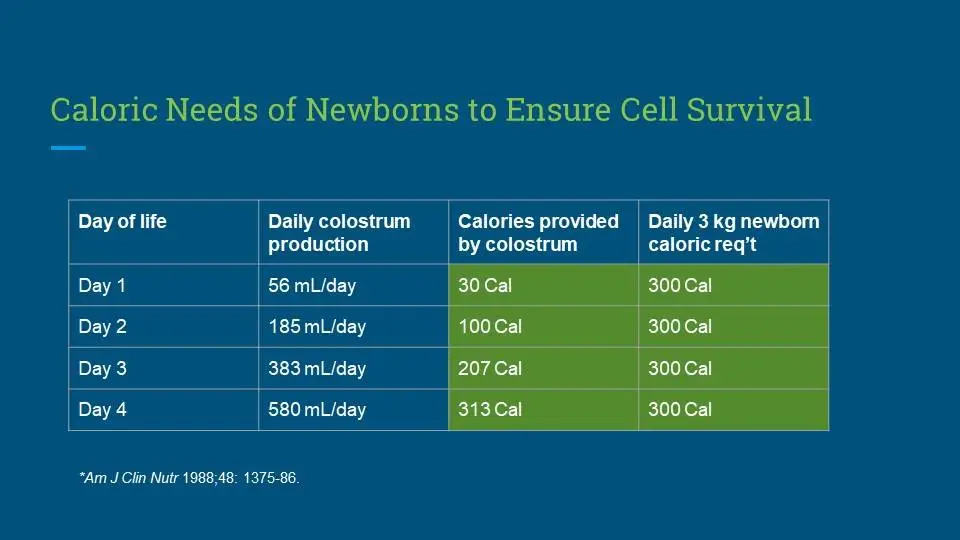
Colostrum Calories
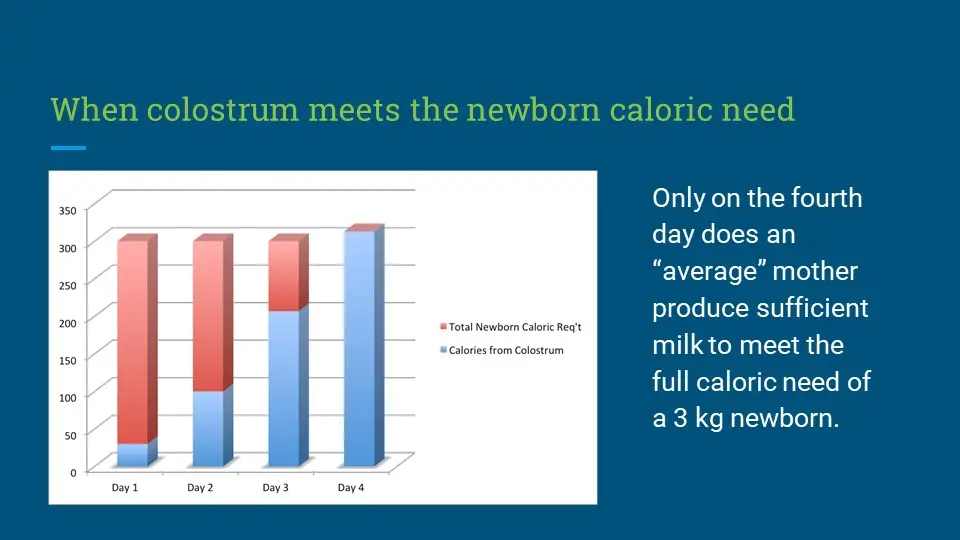
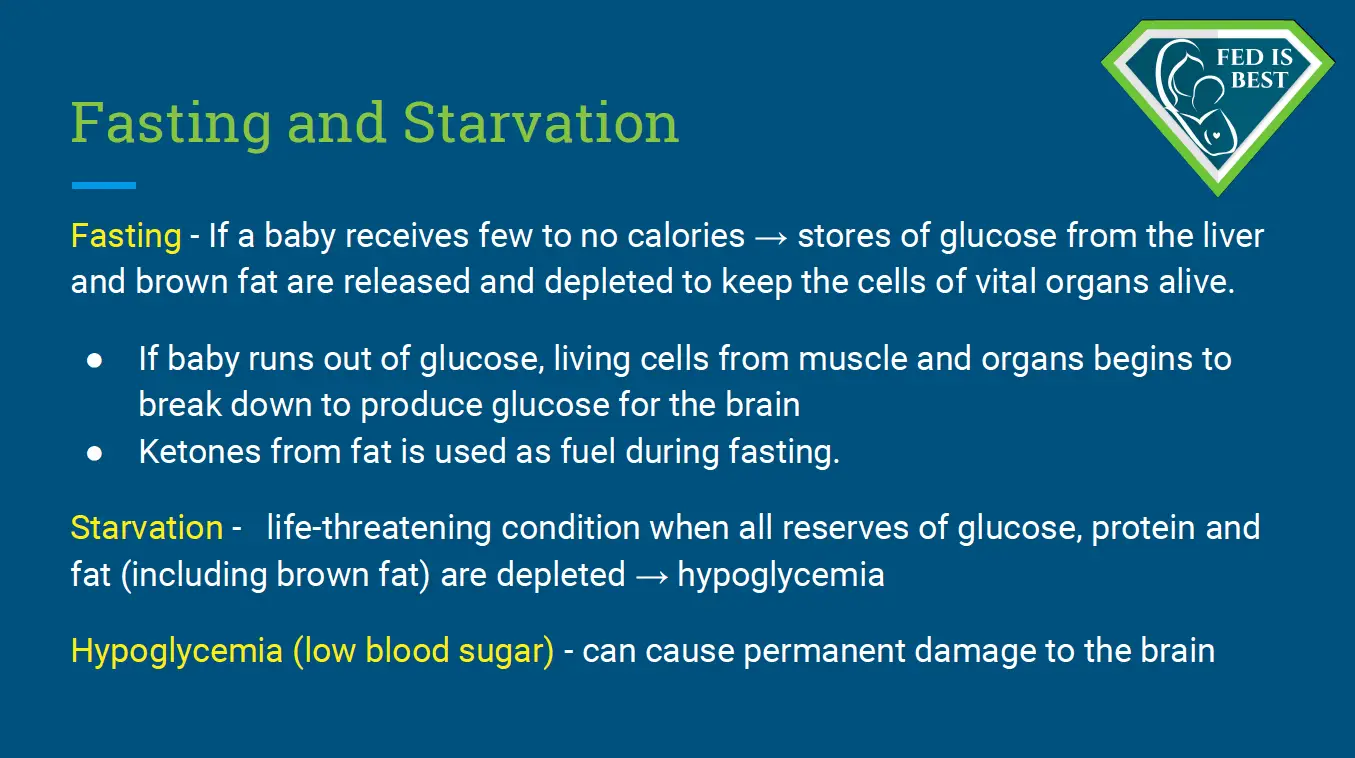
The scientific literature shows that colostrum, in fact, has fewer calories, containing 54 Calories/100 mL compared to 66-77 Calories/100 mL in mature breast milk (Gidrewicz and Fenton, 2014). Therefore, in the period before lactogenesis II, an exclusively colostrum-fed newborn is “fasting,” meaning that the baby is consuming fewer calories than she is expending, causing weight loss. Babies are dependant on their metabolic reserves until the onset of copious milk production. However, some babies do not have enough reserves and this can result in acute starvation-related complications. These complications can result in irreversible impairments in brain development. The term “starvation” is not intended to be inflammatory; it is a medically accurate diagnosis, the definition of which is explained below.
Complications From Insufficient Breast Milk Research:
Research has shown that among healthy term newborns who are discharged from the hospital, exclusively breastfed newborns are twice as likelyto be readmitted to the hospital, most commonly for hyperbilirubinemia and dehydration. They are also more likely to require more follow-up visits with their pediatricians for concerns related to feeding and adequate weight gain. (Flaherman et al., 2018).
A study from the U.K. showed that among healthy term and near-term newborns, exclusive breastfeeding at discharge doubled the risk for readmission for hypoglycemia (Dassios et al, 2018).
According to a review published in the Journal Of Family Practicein June 2018, “exclusive breastfeeding at discharge from the hospital is likely the single greatest risk factor for hospital readmission in newborns. Term infants who are exclusively breastfed are more likely to be hospitalized compared to formula-fed or mixed-fed infants, due to hyperbilirubinemia, dehydration, hypernatremia, and weight loss.” They estimated that for every 71 infants that are exclusively breastfed, one is hospitalized for serious feeding complications.
Beyond the first days of life, low breast milk production and the inability to produce a full milk supply are common.
Data from the Infant Feeding Practices Study showed that 12% or one in eight women were unable to maintain a breastfeeding relationship for the first year of life. Those most commonly affected were women with high BMIs and women with high depression symptoms (although it is unclear whether the depression is the cause or the effect of failed lactation; Stuebe et al., 2014).
The largest study ever done to measure actual breast milk production was done by Kent et al. in 2016 following 116 breastfeeding mothers with and without breastfeeding problems. The mothers measured all the breast milk they fed their infants over the first month of life through direct feeding (using weighted feeds) and expressed breast milk feeding. This study found that between days 11 and 13, 2/3rd of the mothers could not produce more than the minimum 440 mL required to feed their infant exclusively and between 14 and 28 days, nearly 1/3rd could not produce that minimum. This study likely over-represented mothers will low milk supply given that the study required intensive daily test weighing and logging of pumped milk volumes. However, this is off set by the fact that the investigators defined “low milk supply” as less than 440 mL/day, the amount that is just enough to meet a 2.64 kg or 5.8 lb baby’s daily caloric need (at 110 calories/kg/day). With many babies requiring much more than 440 mL/day at the end of 4 weeks, this aspect of the study underestimated the number of infants who are truly not getting their full requirement and who are likely showing signs of persistent hunger.
Dr. Marianne Neifert, Clinical Professor of Pediatrics at the University of Colorado Denver School of Medicine, co-authored a 1990 study of 319 breastfeeding primiparous (first-time) mothers and found 15% were unable to produce sufficient milk by three weeks after delivery despite intensive lactation support.
In a study of 1065 mothers, 532 or 50% had breastfeeding-related problems. Thirty-one percent affected the mother (e.g., engorgement, fissures, low milk supply, infections, breastfeeding cessation), and 10% affected the newborn (poor suction, neonatal jaundice, pathological weight loss, need for hospital admission). Nine percent affected both the mother and the newborn (Govonni, Richi, 2019). Among the identified risk factors for breastfeeding problems, operative vaginal deliveries and cesarean delivery had the highest associated risk for breastfeeding problems. Other factors like higher maternal age, number of previous deliveries, and lower Apgar scores also increased the risk of DOLII.
Dr. Shannon Kelleher talks about these staggering numbers in her publication, “Biological underpinnings of breastfeeding challenges: the role of genetics, diet, and environment on lactation physiology,” in which she says the prevalence of lactation insufficiency may be much higher, as women internationally cited that their baby was “not satisfied with breast milk” as the primary reasons for weaning prior to 6 months.
Listening to Mothers
The data show that maternal perception of insufficient breast milk and the onset of lactogenesis II is in fact accurate. Listening to the mother instead of encouraging her to distrust her own instincts is critical to helping her reach her breastfeeding goals and maintaining her confidence.
The study called “Maternal Perception of the Onset of Lactation Is a Valid, Public Health Indicator of Lactogenesis Stage II” showed that maternal perception of onset of lactogenesis II (including cases when they are delayed) is valid. Since small volumes of colostrum cannot sustain an infant long-term and prolonged exclusive colostrum feeding can result in complications, maternal perception of onset of copious milk production can be used to determine whether or not an infant’s signs of distress are due to persistent hunger. Infants showing distress before the onset of lactogenesis II are at high risk for feeding complications.
Despite the lack of evidence using the gold-standard of randomized controlled trials (RCTs) showing that supplementation interferes with breastfeeding, health professionals and parents continue to be taught to avoid supplementation until an infant has developed or is at serious risk of insufficient feeding complications. In fact, six RCT studies have shown that in infants with weight loss above the 75th percentile, judicious supplementation with 10 mL (two teaspoons) of donor breast or formula milk after nursing had no effect on long-term breastfeeding, one showing it prevented hospital readmissions in all of the supplemented newborns.
Dr. Flaherman’s research suggests that it is not simply early supplementation that affects breastfeeding outcome, but the volume, delivery mode, and rationale for use that are important. She also suggests that reverse causation may be a factor in breastfeeding cessation in that breastfeeding problems lead to formula use, rather than formula use causing breastfeeding problems. Concerns about limited amounts of formula sensitizing the infant‘s “virgin gut” are speculative and pale in comparison to the risk of brain damage from insufficient food and fluids.
It is unconscionable to scare mothers into withholding supplements while not disclosing the risks of insufficient milk. Would we be even having this conversation if banked donor milk were available for all babies who needed temporary supplementation?
Because of this research, it’s imperative to assess each mother and baby to identify potential individual risk factors for delayed onset of lactogenesis II or low milk supply. This will help the health care team offer timely, temporary supplemental nutrition with banked donor milk or formula milk to prevent complications while providing optimal lactation management and support for identified high-risk dyads. Additionally, the health care team can identify scant or absent colostrum in a high-risk mother through instruction on the manual expression of colostrum.
A comprehensive clinical exam/assessment by the pediatrician, nurse, and lactation consultant care team is necessary every eight hours to evaluate every newborn for safe and adequate intake while breastfeeding, and the mother’s observations should be part of the evaluation. The pediatrician, nurse, LC, and parents should have clearly defined roles in the treatment plan.
The health care team should be evaluating the newborn for:
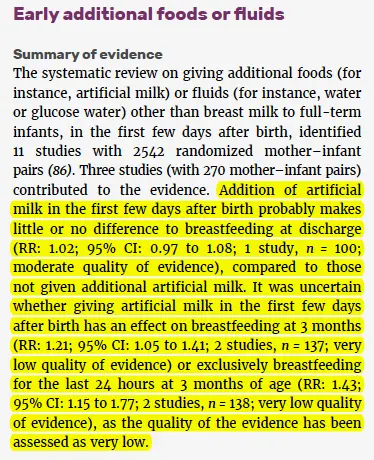
In 2017, the World Health Organization published its guidelines updating its recommendations for“Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services,”which outlines the evidence for the WHO recommendations on breastfeeding support for newborns in health facilities based on the Ten Steps to Successful Breastfeeding. Here is the evidence presented to justify the recommendation to avoid supplementation in breastfed newborns.
How did the very low quality of evidence turn into moderate-quality evidence for exclusive breastfeeding, particularly when the evidence showed improvement of breastfeeding rates in supplemented breastfed newborns?
7. Do you believe exclusive breastfeeding is a good goal to promote?
We do if a mother wants to exclusively breastfeed and they are fully informed about their individualized risk factors for delayed onset and or potential low milk supply. We promote and educate families about safe exclusive breastfeeding because no other health organization informs parents about the risks of insufficient feeding complications and how easy they are to prevent. To be fully informed, parents must be educated about both the benefits and risks of exclusive breastfeeding. Currently, they are only taught about the benefits and not the risks.
Many mothers want to exclusively breastfeed, and day after day in our support group we help mothers achieve this goal by developing an actionable breastfeeding plan that works for their unique needs. Mothers, especially first-time mothers, have told us that they gave up breastfeeding in the days after birth because they felt that they were not making enough milk, when in fact, their milk arrival was simplydelayed.
If these mothers were educated about their risk factors for delayed onset of milk or insufficient milk supply, how to safely supplement while waiting for their milk to come in, how to increase their milk production, or how to sustain a combo-feeding relationship if their supply is limited, they could go on to have a sustainable breastfeeding relationship instead of losing confidence and stopping breastfeeding altogether.
Our actionable breastfeeding plan provides guidelines for protecting the mother’s milk supply if temporary supplementation is necessary. It’s not true that supplementing decreases the milk supply if a mother’s breasts are adequately stimulated and emptied while supplementing breastfeeding.
Responsiblebreastfeeding education requires families to be taught when to offer safe supplementation of expressed breastmilk or properly prepared formula to protect their baby’s health in the case of insufficient breast milk supply or intake. In some instances, the need for supplementation cannotwait for the consultation with a pediatrician or lactation consultant as doing so may result in serious harm. Many mothers have told us they panicked when they needed to purchase formula and they didn’t know how to safely prepare it or how much to give.
While we do support safe exclusive breastfeeding, we also recognize that some mothers find that it is not working for them or their babies. In those cases, we believe it is important to provide a mother with all of her feeding options, as opposed to encouraging only continued exclusive breastfeeding. Mothers tell us they do not feel heard when there is a clear agenda to support only exclusive breastfeeding. We will support her in her choice, whether that is exclusive breastfeeding, exclusive formula feeding, or a combination. If she states that continued exclusive breastfeeding is important to her, then it is important to us also. We support her feeding goal while prioritizing her infant’s health and safety by recommending supplementation with milk bank donor milk or formula if needed before unsafe conditions occur.
As health care professionals, it is our ethical duty to provide families with all of their options, and exclusive breastfeeding is no exception. We believe the exclusive breastfeeding metric needs immediate reform in light of the current data regarding harm and lack of data showing efficacy. The practice guidelines also need to reflect the need to respects maternal choice. A new alternative to the Baby-Friendly policy is the new Family-Friendly Protocol at Rush Foundation Hospital, whose philosophy is to improve patient outcomes by respecting parental choice to breastfeed, combo-feed or formula feed while providing all the education and support needed to achieve individual feeding goals.
8. If you believe exclusive breastfeeding is an important goal, why are you not promoting it as the ideal or best?
We believe a fully fed baby is the ideal, and for the mothers who are not making enough milk, supplementation with banked donor milk or formula is ideal and best infant feeding. An infant who is exclusively breastfed and is not safely or sufficiently fed is neverideal or best.
When we started our first Facebook page it was titled “Breast is best, if you have enough breast milk.” Mothers started messaging us with their own heartbreaking stories and we’ve taken to heart the thousands of letters we have received from mothers describing the pressure they felt to achieve the “ideal” of exclusive breastfeeding from birth to 6 months, and thefear they have that formula will hurt their babies’ health and future potential. They describe suffering from unbearable shame and guilt when it was not possible for biological, economic, psychological, and/or other personal reasons. Parents told us they desperately needed to hear a more inclusive infant feeding message.The suggestion to change our phraseology from “Breast is best if you have enough breastmilk” to “Fed Is Best” was heard, and this is how #FedIsBest was born. It was the right thing to do.
As the Foundation has grown, we quickly learned that mothers are under the impression that low or delayed milk supply is rare. This puts mothers in a position where they feel they have failedor that they are somehow biologically “abnormal” when they were not producing enough milk, even when they have followed the advice of their lactation professionals. They also feel alone because of how breastfeeding education downplays the prevalence of insufficient milk.
Sadly, mothers have told us they knew their babies were hungry but were taught that feeding their babies formula milk is very harmful when the true harm comes from not feeding their baby enough!Isn’t the first rule in lactation support “feed the baby”? It’s not “push the baby to the limits of his tolerance to avoid a few milliliters of donor milk or formula.”
Parents have unknowingly harmed their infants under the guidance of their lactation educators and health professionals. Some of these mothers lose trust in breastfeeding altogether, which is not what any of us want.
Every lactation consultant knows that if a baby is not getting enough to eat, temporary donor milk or formula supplementation can help breastfeeding, not harm it. Mothers have the right to know and should be empowered with a supplementation plan in case they need it. To do otherwise is to hide the truth and while making mothers dependent on expert help that they may not have access to in the time required to prevent harm.
Having a Plan B does not destroy mothers’ confidence in their bodies; it gives them the confidence to know they can care for their babies no matter what happens, and it gives them the knowledge they need to support their milk supply until the breastfeeding problem can be addressed.
9. Cluster feeding is a well-known phenomenon. Why would you say it’s a sign of the baby not eating enough? The LLL describes the “second-night syndrome” as normal, why do you say it’s not?
Cluster feedingcan be normal when it lasts for a few hours once a day and the baby becomes satisfied after several short feedings. The Academy Of Breastfeeding Medicine defines cluster feeding as “several short feedings close together.” However, mothers are being told constant and prolonged feeding around the clock is “cluster feeding,” and this is where confusion that can result in harm begins. There is a point when cluster feeding becomes a clear sign of insufficient breast milk and/or insufficient transfer of milk, and those signs must be taken seriously for the health and safety of the infant. Mothers tell us they receive conflicting information and as a result, they become very frustrated, lose confidence and want to stop breastfeeding. Or, they persist with exclusive breastfeeding due to incorrect advice, and negative outcomes occur.
It is important to define what cluster feeding really is as health professionals and evaluate and intervene when an infant is in danger of insufficient feeding complications.
There is no stronger maternal drive than to feed your baby and protect him from harm. Mothers experience incredible emotional suffering when they are told their baby “was just cluster feeding,” but it turns out in hindsight they were not eating a sufficient amount, even after nursing for hours. They blame themselves rather than the health professionals who should have taken their concerns seriously.
The “Second Night Syndrome” may be common, but this does not imply that it is normal, safe or ideal. In fact, there has never been a single study documenting the safety of “Second Night Syndrome,” which we know has led to critical illness and injuries in breastfed infants who were not supplemented in a timely or adequate fashion. Our Co-Founder Jody, wrote about the Second Night Syndrome drawing from years of clinical experience working in the Nursery/NICU to inform the article. Some breastfeeding mothers talk about the “Second Night Syndrome” by describing itas absolute hell!They describe their babies as nursing non-stop and as soon as they take baby off the breast they cry frantically. The only time their babies are not crying is when they are breastfeeding. Some mothers say their babies even cry while frantically nursing and nothing consoles them. This is neither safe nor humane to the mother, who is recovering, and the baby who has to endure prolonged hunger. Such conditions not only increase the risk of feeding complications and admissions, but it can also result in accidental bed-sharing and infant falls or suffocation, known as Sudden Unexpected Postnatal Collapse.
The second night of your baby’s life should never be hell. If your baby is crying non-stop despite adequate breastfeeding, an immediate physical assessment by the RN or MD should be made to determine why your baby is crying and if immediate supplementation is necessary.
A check of their glucose, bilirubin, weight and possibly their electrolytes should be performed by a nurse, physician or nurse practitioner to assess whether a newborn is being sufficiently fed and whether supplementation is needed to protect your newborn. Research tells us that 1 in 5 mothers have delayed onset of full milk production, so we simply cannot ignore the abnormal behavior of a non-stop crying baby, knowing there will be babies who need to be supplemented.
Furthermore, the exclusive breastfeeding quality metric has never been proven in randomized, controlled trials to improve breastfeeding rates, while decades of evidence have shown that rigid insistence on this metric increases the risk of harm.
THANK YOU FOR YOUR INTEREST IN THE FED IS BEST FOUNDATION!
Our mission statement is:
The Fed is Best Foundation works to identify critical gaps in current breastfeeding protocols, guidelines, and education programs. We provide families and health professionals with the most up-to-date scientific research, education, and resources to practice safe infant feeding with breast milk, formula, or a combination of both. To be fully informed, parents must be taught about the risks of insufficient breast milk intake while supporting exclusive breastfeeding in order to eliminate preventable hospitalizations for insufficient feeding complications. Finally, we strive to eliminate infant feeding shaming while prioritizing perinatal mental health.
HOW YOU CAN SUPPORT FED IS BEST
There are many ways you can support the mission of the Fed is Best Foundation. Please consider contributing in the following ways:
Join us in any of the Fed is Best volunteer and advocacy, groups. We currently have– Health Care Professional Advocacy Group, Advocacy Group, Research Group, Volunteer Group, Editing Group, Social Media Group, Legal Group, Marketing Group, Maternal Mental Health Advocacy Group, Private Infant Feeding Support Group, Global Advocacy Group, and Fundraising Group. Please send an email to Jody@fedisbest.org– if you are interested in joining any of our volunteer groups. For our health professional advocacy group, join us here.
If you need infant feeding and parenting support, we have a support group– Join us here.
Make a donation to the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign theFed is Best Petition at Change.org today, and share it with others.
Share the stories and the message of theFed is Best Foundation through word-of-mouth, by posting on your social media page and by sending our FREE infant feeding educational resources to expectant moms that you know. Share the Fed is Best campaign letterwith everyone you know.
Print out ourletter to obstetric providers and mail them to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
Write your local elected officials about what is happening to newborn babies in hospitals and ask for legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
Send us your stories. Share with us your successes, your struggles and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
Send us messages of support. We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
Shop at Amazon Smileand Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!
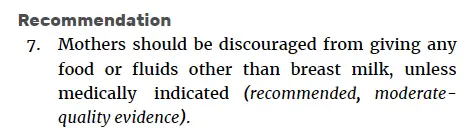
The WHO health policy that has been responsible for millions of preventable hospital admissions of newborns for insufficient feeding complications is Step 6 of the Ten Steps to Successful Breastfeeding: “Give no additional food or fluid other than breast milk unless medically indicated.” Complications of insufficient feeding from exclusive breastfeeding before copious milk production are now among the leading causes of newborn extended and repeat hospitalization, namely jaundice (hyperbilirubinemia), dehydration and hypoglycemia.
In 2017, the World Health Organization published its guidelines updating its recommendations for “Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services,” which outlines the evidence for the WHO recommendations on breastfeeding support for newborns in health facilities based on the Ten Steps to Successful Breastfeeding. Here is the evidence presented to justify the recommendation to avoid supplementation in breastfed newborns.
The WHO guidelines authors went on to conclude the following:
How did very low quality of evidence turn into moderate-quality evidence for exclusive breastfeeding particularly when the evidence showed improvement of breastfeeding rates in supplemented breastfed newborns?Continue reading →