
Frequent breastfeeding and cluster feeding are often used interchangeably, creating confusion for parents. This educational blog will help parents clarify the differences between the two.
What are the differences between frequent breastfeeding and cluster feeding before lactogenesis II for newborns?
Frequent Feeding-Newborn babies feed frequently (every 2-3 hours) before lactogenesis II, the onset of copious milk production. Frequent feeding is expected and normal.
Cluster Feeding-Cluster feeding occurs after the arrival of lactogenesis II and is defined as a series of short feeding sessions lasting 2-3 hours daily.
The Academy of Breastfeeding Medicine supplementary feeding protocol states cluster feeding before lactogenesis II requires a prompt evaluation to determine if the baby is getting enough colostrum.
An evaluation includes the following:
- It is essential to determine if colostrum is present by hand expression before and after nursing.
- The baby requires an observed feeding session, during which the position and latch must be evaluated to ensure that colostrum is transferred effectively and the baby is nursing effectively.

Note* The onset of LII timing varies between mothers, but it’s expected before 72 hours after birth. Lactogenesis II is delayed if copious milk production does not arrive within 72 hours.
This checklist will help you determine whether your baby’s feeding behavior is normal after birth and ensure your newborn receives adequate fluids and colostrum.
| Normal Frequent Feeding | Abnormal Feeding Behavior Before Lactogenesis II |
| It is common: Breastfeeding every 2-3 hours, or 10-12 times in 24 hours. | The baby is nursing more than every 2 hours or is unsettled, fussing, or crying after nursing. May show signs of low blood sugar levels with hand tremors or high-pitched crying. Some babies become exhausted from excessive feeding and crying, eventually appearing fatigued and uninterested in feeding. *Review maternal medical and psychosocial history to evaluate DOL2 risk factors to provide timely supplementation. |
| Baby is nursing effectively on both breasts and is satisfied after nursing and in between feedings. | Baby continues exhibiting strong HUNGER cues after nursing and between nursing sessions. The mother is concerned and distraught. |
| Appropriate wet and dirty diapers | Concentrated dark urine, reduced urination (no wet diapers for 6 hours), reduced bowel movements/meconium, and urate crystals in the diaper (orangish to red staining after urination) |
| Lips, mouth, and tongue are moist. Ample oral saliva. | Lips may be cracked, dry, or peeling.The mucosal membranes(mouth and tongue) are pasty or dry, with scant saliva. |
| Jaundice levels (yellow skin) are stable and within normal limits. | Jaundice levels are increasing, and the eyes are yellow. |
| Weight loss is not more than 4.5% in the first 24 hours of life, 7% on day 2, or more than 7% at any time. *We recommend using an online weight loss nomogram that tracks hourly weight loss for the optimal tracking Newt – Newborn Weight Loss Tool | Weight loss is more than 4.5% in the first 24 hours of life and more than 7% on day 2. *We recommend using an online weight loss nomogram that tracks hourly weight loss for optimal tracking Newt – Newborn Weight Loss Tool |
| Does not warrant serum blood testing. | Abnormal serum laboratory results for dehydration, hypoglycemia, or hyperbilirubinemia. |
What if your baby is exhibiting abnormal feeding behavior?
It’s important to note that delayed onset of lactogenesis is common (at least 1 in 5 moms). This research suggests that the prevalence of delayed onset of lactogenesis II (milk coming in) has reached epidemic proportions in the United States, and there will be babies who require temporary supplementation while waiting for the arrival of an adequate milk supply. Parents should be reassured that temporary supplementation does not derail breastfeeding. In fact, 6 studies have shown that judicious supplementation did not affectlong-term breastfeeding. One study showed it prevented hospital readmissions in all of the supplemented newborns. Another showed it actually helped sustain breastfeeding.

Click here to learn why the second-night syndromeis abnormal.
Parents must be taught about inadequate feeding, how to supplement if necessary, and how to maintain a milk supply while determining the cause. They should be assured that temporary supplementation does not derail breastfeeding. In fact, studies show supplementation is a tool for achieving exclusive breastfeeding. There have now been six studies showing that supplementation with two teaspoons (10 mL) of formula or donor breast milk after nursing did not affect long-term breastfeeding. One study showed it prevented hospital readmissions in all of the supplemented newborns. Another showed it actually helped breastfeeding.
How to supplement:

Click hereto learn how to supplement your baby.
To learn more about cluster feeding, click here.
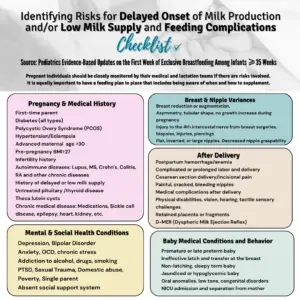
Note: A mother’s medical and psychosocial history should be reviewed during pregnancy to assess DOL II risk factors. Knowing your risk factors for DOLII or low milk supply might be overwhelming. Looking at a list of risk factors might be overwhelming, but no matter your risk factors, risk only means a problem might happen, not that it will. However, you will be prepared and know how to keep your baby safe following our supplementing/feeding guidelines.
Additional resources:
https://fedisbest.org/2024/03/the-fed-is-best-book-protecting-infants-and-empowering-choices/
Newt – Newborn Weight Loss Tool
ABM Clinical Protocol #3: Supplementary Feedings in the Healthy Term Breastfed Neonate,
Is the “breast is best” mantra an oversimplification? – PubMed (nih.gov)ed 2017 (bfmed.org)
Is the “breaRehospitalization for Neonatal Dehydration: A Nested Case-Control Study |
Neonatology | JAMA Pediatrics | JAMA Network
https://fedisbest.org/2018/10/feeding-your-baby-when-supplementing-saves-breastfeeding-and-lives/
https://fedisbest.org/resources-for-parents/feeding-plan/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9325457/