Written by Dr. Ruth Ann Harpur, Clinical Psychologist
Current guidelines from the World Health Organization (WHO) encourage women to exclusively breastfeed their babies for six months and to continue to breastfeed, alongside introducing solid foods, throughout the first year and beyond. These guidelines are adopted by major health authorities throughout the world, and millions of pregnant women are unilaterally encouraged to follow them.
However, the WHO standard is clearly not attainable for all women, as is borne out by the data. Despite the fact that most women initiate breastfeeding, only a minority will attain the six-month standard. For example, in the UK, only seventeen percent of women are exclusively breastfeeding at three months, and by six months, only thirty-four percent of babies are receiving any breast milk at all (Infant Feeding Survey 2010). In the US, 44 percent of babies are exclusively breastfed at 3 months, and at 6 months, 22 percent of babies are exclusively breastfed.
Current research shows that women who intend to breastfeed but subsequently turn to formula, are at particularly high risk for postnatal depression (Borra et al., 2015). Interestingly, the paper also indicates that women who don’t intend to breastfeed, but who breastfeed anyway, are also at increased risk for postnatal depression.
Whatever the reasons women turn to formula, studies examining the experiences of these women consistently report feelings of guilt, anger, worry, uncertainty, and a sense of failure. At the same time, these mothers also reported a sense of relief when formula was introduced (Lakshman, Ogilvie, & Ong, 2009).
We do not yet have a solid evidence-based understanding of why this link exists, as the relationship between feeding experiences and postnatal mental health issues is likely to be complex and different for different women. However, one thing is for sure, there is a huge human and emotional cost for many women and their families when breastfeeding doesn’t work out. Stories such as this one, Postpartum & Motherhood: Battle Wounds & Badge of Honour which Masumé has generously shared, speak to these costs, show that these women are not alone, and, thankfully, give hope that recovery is possible and motherhood can be fully enjoyed and embraced with or without breast milk.
However, I think we need to ask ourselves, as a society, and especially for those of us who work in healthcare, if there is a different way. My experience as a mother and as a clinical psychologist has led me to believe that our current definition of “success” and “failure” is a large contributor to the psychological distress many mothers experience when they are unable to realize their hopes for how they feed their babies.
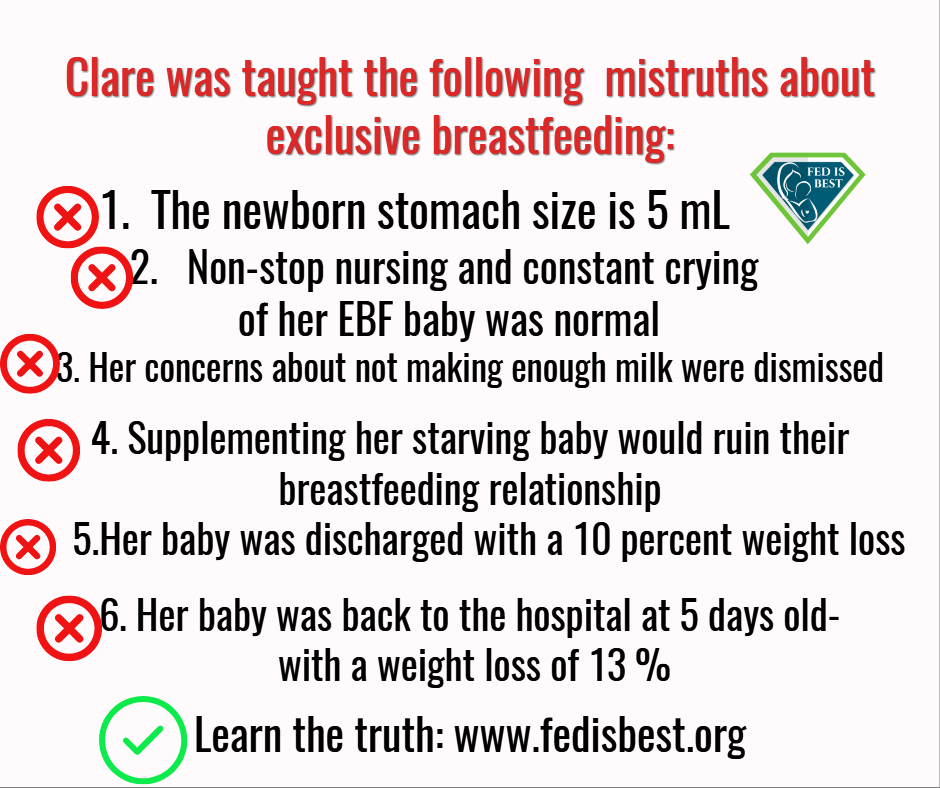
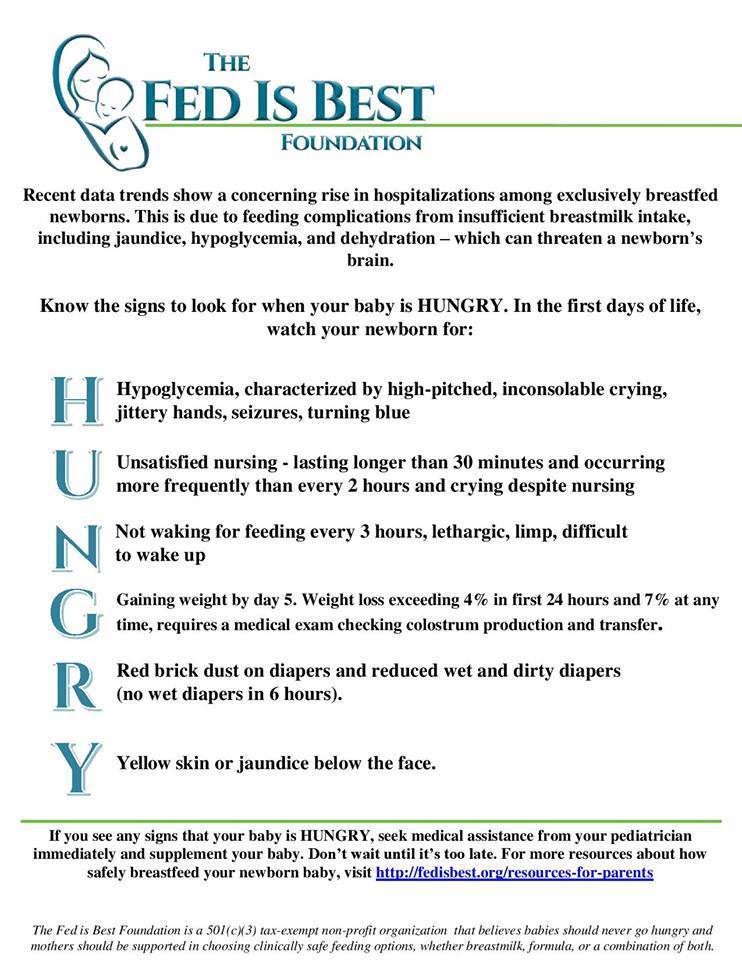
First, I think we need to recognize that the WHO standards are clearly not attainable or safe for all women and babies. Some newborn babies experience serious feeding-related complications in an attempt to reach this exclusive breastfeeding standard. Evidence shows up to one in five new mothers will experience delayed onset of mature milk, while an unknown amount mothers never establish lactation. Pushing exclusive breastfeeding in the face of these realities puts newborns at risk for feeding-related complications ranging from hyperbilirubinemia, hypoglycemia to acute dehydration, and even death. For some babies, supplementation is literally life-saving, and yet their mothers still feel a sense of failure for not achieving the prescribed breastfeeding standard.
I propose we collectively redefine successful feeding to take into account the unique needs of each mother, baby, and family. Rather than focusing on the feeding process, we should set goals that prioritize healthy outcomes for families and which are attainable through all available safe feeding methods.
I was particularly inspired to write this article because of the many mothers within The Fed is Best Foundation’s private support community who have experienced difficulties while breastfeeding their first baby, and are confused and torn as to whether or not to try again with a second child. As an expert in mental health, I feel we must help parents set realistic goals that allow them to feel positive, confident, and supported in the process of nourishing their baby.
1) The first and foremost healthy and attainable feeding goal is a fully nourished, thriving, and satisfied baby.
If your feeding method of choice isn’t keeping the baby fully nourished, then it’s time to do something about it. Maybe you started out breastfeeding, but the baby is showing signs of hunger. This can be assessed using The Fed Is Best Foundation’s HUNGRY guidelines. If we revise the unrealistic goal of exclusive breastfeeding for every woman to the goal of a nutritionally satisfied baby, then making the informed choice to supplement with expressed breast milk or formula becomes a positive solution to a problem instead of a negative indication of failure.
That said, the act of feeding a baby provides more than physical nourishment. It also brings comfort, family, community, sharing, and bonding, and perhaps never more so than when nourishing a newborn eight to twelve times per day.
2) This brings us to the second healthy and attainable feeding goal: for mother and baby to feed in comfort.
There’s no getting around it. Some babies take to breastfeeding like a duck to water. Others need a little help in learning to suck effectively. Mothers need time and support to learn breastfeeding positions that work both for themselves and their baby. Some babies experience gas and reflux, and those babies may need some help to feed comfortably. Sometimes, no matter how much support is given, a mother will experience breastfeeding as painful, or a baby will be unable to attain a good enough latch to suckle effectively.
If breastfeeding is not comfortable for you, as a mother, then take action. Get help with latch and positioning, and seek medical advice for possible conditions that may interfere with comfort while breastfeeding.
Sadly, some women find breastfeeding so uncomfortable that they begin to dread feeding sessions. Preserving through constant pain and discomfort helps absolutely nobody and may threaten the bond between mother and baby. This is an urgent reason to re-evaluate feeding methods. A baby needs to be fed with love and comfort, not through a mother’s tears or gritted teeth.
For instance, if a mother finds direct breastfeeding too mentally or physically painful to continue, but still wants to provide some breast milk, then expressing milk may be an option. Pumping can work for some women, or it can become too emotionally and physically demanding for others. Time spent with a mechanical pump is time in which a mother is unable to rest and possibly unable to spend time with her baby or other children. If pumping doesn’t work for a particular woman or family, then, sometimes, the best thing is to let go of that goal without guilt.
3) The third healthy and attainable feeding goal is for the mother to be fully present and emotionally available to the baby, older children, and/or partners.
This really does come down to individual families and what they need, given their particular circumstances. However, being emotionally available to the family unit requires at least a reasonable amount of sleep, management of physical pain, and treatment of any physical or mental health conditions.
For some women, breastfeeding is a very positive and fulfilling experience that enhances family life. For others, it has a negative and draining effect on the family dynamic for a variety of reasons. More individualized approaches are beneficial, as any number of issues may arise for which a re-evaluation of the goals is required in order to maintain everyone’s emotional and physical wellness.
For example, if a mother feels her mental health is impacted by sleep deprivation, a partner can give a night time bottle feed to allow mum to get some much-needed rest. I have worked with women for whom a full night’s sleep is essential for that mother’s mental health. Under such circumstances, a partner helping with night feeds becomes vitally important. Breastfeeding may still be possible with expressed milk or supplementary formula given at night, however, we should keep in mind that the goal is not exclusive breastfeeding, but rather, a happy and functional family.
Other mothers wish to breastfeed, but then find that their mental or physical health must take priority. Sometimes the best thing is for a mother to fully formula feed in order to take medication that is incompatible with breastfeeding. This is an entirely reasonable thing to do. A mothers’ physical and mental health matters to them, to their partners, and to their children. Nobody benefits from a mother who is suffering, least of all a baby who needs, above all else, to feel loved and enjoyed by their family.
Each mother and each family needs to consider their own circumstances and determine what is a priority for them.
I encourage parents to set aside the WHO recommendations, and instead take up these three feeding goals of a fully physically nourished baby, a comfortable feeding relationship, and a mother that feels emotionally available for her family. These goals are attainable regardless of which (clinically safe) method you use to get there.
By changing how we define successful infant feeding, we can empower families to feel positive and confident about how they nourish their babies, and we may prevent the psychological stress which results when things don’t go according to plan.
We must recognize that a feeding method is successful when a mother is comfortable and relaxed, and she is confident her baby is nourished. Successful feeding is a fully fed baby who knows he or she is loved and nourished, physically and emotionally, in a calm, healthy, and happy family.

Ruth Ann holds a Ph.D. in developmental psychology from the University of Southampton and a Doctorate in Clinical Psychology from the University of East Anglia. After unexpectedly turning to formula to feed her daughter, she came across The Fed is Best Foundation and was moved and disturbed by the level of psychological distress, depression, anxiety, and trauma which many women reaching out to The Foundation are experiencing. An expert in mental health, she is passionate about empowering women to confidently nourish themselves and their baby, whatever their feeding method.
HOW YOU CAN SUPPORT FED IS BEST
There are many ways you can support the mission of the Fed is Best Foundation. Please consider contributing in the following ways:
- Fundraising Group. Please send an email to Jody@fedisbest.org if you are interested in joining any of our volunteer groups.
- If you need infant feeding support, we have a private support group– Join us here.
- If you or your baby were harmed from complications of insufficient breastfeeding please send a message to contact@fedisbest.org
- Make a donation to the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing, and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
- Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign the Fed is Best Petition at Change.org today, and share it with others.
- Share the stories and the message of the Fed is Best Foundation through word-of-mouth, by posting on your social media page, and by sending our FREE infant feeding educational resources to expectant moms that you know. Share the Fed is Best campaign letter with everyone you know.
- Write a letter to your health providers and hospitals about the Fed is Best Foundation. Write to them about feeding complications your child may have experienced.
- Print out our letter to obstetric providers and mail them to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
- Write to your local elected officials about what is happening to newborn babies in hospitals and ask for the legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
- Send us your stories. Share with us your successes, your struggles and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
- Send us messages of support. We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
- Shop at Amazon Smile and Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!

Click here to join us!