BY ALEXANDRIA FISCHER, PHD CANDIDATE AT THE RENSSELAER POLYTECHNIC INSTITUTE, STUDYING SYNTHETIC MICROBIAL COMMUNITIES
The “magic” of breastmilk is never-ending, plastered everywhere on social media with little regard to true scientific analysis. The idea that breastfeeding prevents cancer is a huge promotion point for why mothers should breastfeed at all costs. But while the cancer-preventing benefits are overblown, there is an even bigger claim surrounding the anti-cancer properties of breastmilk; that breast milk kills cancer, in and of itself. This is a claim that I have seen made many times, so I decided to dig into the research and see where this claim came from and how truthful the claim is.
So where did this idea that breastmilk can kill cancer cells come from? It’s actually a long, and interesting accident of science. In 1995 researchers were studying the adherence of bacteria to lung cancer cells in the presence of human milk fractions [1]. Fractionation is simply the process where the different molecule types in any substance are separated from one another. One of the tested fractions showed not only inhibition of bacterial adherence but also induced apoptosis of the tumor cells. Apoptosis is just a fancy word for cell death. This fraction was α-lactalbumin, an abundant protein in milk. However, α-lactalbumin in its natural state has no effect on tumor cells. So what happened in the 1995 study? It seems that the researchers fractionated the milk at a low pH (acidic) implying that there was some kind of change in the structure of the protein. Further work showed that a reaction between the α-lactalbumin and oleic acid (acids lower pH) form the HAMLET compound [2]. HAMLET stands for Human α-lactalbumin Made LEthal to Tumors. HAMLET is an incredibly interesting compound that induced cell death (apoptosis) in cancer cells but not human cells.
As a neonatal nurse practitioner in a community hospital, I see babies in the postpartum unit every day and make decisions about their discharge criteria.
The average length of stay after birth is 24-48 hours for a vaginal delivery and 48-72 hours for cesarean delivery. A lot of information about breastfeeding, newborn care, and post-partum care must be conveyed in that short time, often to new parents who are exhausted and overwhelmed. In an ideal world, every mother-baby dyad would be well suited for breastfeeding. Many women are able to breastfeed without difficulty, but for some, it’s a struggle. The majority of mothers are discharged before their milk comes in, which is why discharge criteria include pediatrician follow-up within 24-48 hours and why weight check appointments are critical so that all breastfeeding babies are protected from inadequate milk intake.
“Days two to five are critical days for normal newborns to be seen by their pediatrician,” said Dr. Vicki Roe, M.D., a pediatrician at North Point Pediatrics in Indiana. “They are still losing weight and their jaundice levels could be increasing. A healthy baby can become a very sick baby quickly, and we must monitor them closely to prevent complications.”
Many of us work in “Baby Friendly” hospitals. Requirements for the Baby-Friendly designation include displaying the WHO/Unicef Ten Steps for successful breastfeeding and adhering to these recommendations. It is important to note that Baby-Friendly does not prohibit supplemental feeding in the case of medical necessity; nevertheless, both medical staff and nursing staff often report that they are afraid to violate the Baby-Friendly “rules.” I find it effective to specifically document the condition I am treating when I order supplemental feedings. This makes the plan of care transparent and easy to communicate, ensures accountability, and meets the requirements of certification. The exclusively breastfed baby with excessive weight loss (EWL)requires careful assessment.
Question: Would you consider laboratory testing if a baby has excessive weight loss and the mother’s milk is not in yet to meet discharge criteria?
A weight loss of 7-10 % certainly prompts further feeding evaluation. A physical exam should be performed, looking for clinical signs of dehydration. I would consider ordering aBasal Metabolic Panel (BMP) to evaluate for dehydration, hypernatremia, and hypoglycemia. In some situations, the decision to supplement based on excessive weight loss may be met with pushback; laboratory evidence of dehydration adds weight to the decision and may forestall disagreement. In our facility, we usually dobilirubin (jaundice) screening using a transcutaneous meter at around 24 hours of life; if I were concerned about weight loss, particularly if there were visible jaundice or risk factors, I would repeat the screening. And of course, if the infant’s clinical appearance were of concern, for instance, if the infant were hypotonic or lethargic, aCBC or complete bloodcount and blood culture would be of paramount importance to check for infection.
Question: Do you take into consideration the mothers’ risk factors for delayed onset of milk when considering supplementation?
Absolutely. The considerations I have outlined below are drivers in assessing not only readiness for discharge but also whether there is an indication for supplementation. A healthy infant born at term and appropriate size for gestational age with no complications can endure a couple of days of low volume colostrum feedings while mother’s milk is coming in. I use the analogy of a bear storing up for hibernation when I speak to parents about prenatal stores and normal expectations for breastfeeding. Maternal considerations and infant health status inform the decision of whether supplemental feeding is needed. A lactation consultant may be of assistance iflactogenesis is delayed and can implement interventions such as pumping or adjusting the infant’s latch and positioning. It is important to work as a team; LCs can offer valuable input into the plan of care, but they can’t make decisions without consulting with the pediatrician. When a medical need for supplemental feeding is recognized, an appropriate plan of care must accurately be conveyed and followed by everyone involved in the care of the dyad.
Question: If a mother has IV fluids during labor, do you think babies who have excessive weight loss can lose more weight than the current guidelines from the AAP?
It has been posited that the administration of IV fluid in the intrapartum period can affect neonatal weight loss. The assertion is that IV fluid “plumps up” (i.e., causes edema) of the fetus, leading to an artificially inflated birth weight. Diuresis after birth then causes apparent significant weight loss. But babies are not diuresing after birth, as evidenced by their low wet diaper output in general.
A 2011 study published in Pediatrics (Chantry et al.) sought to examine potentially modifiable factors in excessive weight loss (EWL) in predominantly breastfed newborns. This was a relatively small study of 316 infants with gestational ages between 32 and 40 weeks. The authors looked at a number of factors, including prenatal feeding plan, supplemental feeding, onset/delay of lactogenesis, nipple type, nipple pain, and interventions during labor, including IV fluid administration. They defined excessive weight loss as ≥10% of birth weight by three days of age. Overall, 18% of infants who were exclusively breastfed or received minimal (defined as <60 ml total) supplemental formula had EWL. 19% of exclusively BF infants had EWL; 16% of minimally supplemented infants had EWL, and only 3% of infants who had supplemental feeds of >60 ml total had EWL. To greatly simplify the statistical analysis, the initial analysis showed a number of factors associated with EWL, including higher maternal age and education, hourly intrapartum fluid balance, postpartum edema, delayed lactogenesis, fewer infant stools, and birth weight. Further analysis found only two significant factors: intrapartum fluid balance and delayed lactogenesis. EWL occurred in 30% of EBF/minimally supplemented infants whose mothers had high hourly intrapartum fluid balance, and 10% of those whose mothers had low hourly fluid balance. Around the issue of delayed lactogenesis (defined as not “feeling noticeably fuller” by 72 hours), 35% of EBF/minimally supplemented infants with mothers who reported delayed lactogenesis had EWL; for women who reported no delay in lactogenesis, 8% of EBF/minimally fed infants had EWL.
I can’t help but wonder whether this study failed to see the forest for the trees. A higher fluid balance may be a marker for longer labor and labor complications, which in turn would certainly affect postpartum recovery, fatigue, and lactogenesis. The authors relied on subjective perception by primigravidas as a definition of delayed lactogenesis and reported it as 42%, a much higher prevalence than the usual estimate of 15%. Indeed, the title of this article could have been “Excess weight loss in the first-born breastfed newborns relates to delayed lactogenesis”—not nearly as exciting. The authors themselves advise caution in interpreting weight loss and state that EWL should not be assumed to be fluid loss alone but mayindeed represent insufficient feeding.
A later study by Elroy et al. (2017) also sought to examine whether there is a relationship between EWL, type of fluid (colloids + crystalloids or crystalloids alone), and IV fluid dose. This was a larger study, involving 801 dyads. EWL was defined as >7% of birth weight. In this case, the authors did not find a difference in the rate of EWL associated with the type of fluid given, nor did they find a dose-response relationship between the amount of fluid and EWL. As an aside, they mention the confounding variable of maternal hypotension, which of necessity would require fluid administration, but which could lead to impaired uteroplacental perfusion and fetal acidosis, affecting the vigor of the infant.
So do I think that a 7-10% or greater weight loss is grounds for concern? Absolutely. Ascribing excessive weight loss to maternal IV fluid is disingenuous at best.
While IV fluid may contribute to perceived weight loss, this relationship is by no means established, but the relationship between poor feeding and weight loss is. With the exception of critical infants with certain prenatal conditions, I do not see infants born with perceptible edema.
A comprehensive exam for every breastfeeding dyad will include:
Maternal health. In the aggregate, women giving birth today are older, have higher BMIs, and are more likely to have underlying chronic health conditions or pregnancy complications than women in previous generations. Delayed childbearing means that women may be having children after the age of 35. Older mothers are more likely to have pregnancy and childbirth complications. The obesity epidemic has affected people of all ages and socioeconomic strata; obese women may have underlying chronic health problems such as diabetes and hypertension and may have more difficulty with mobility and healing. Long or complicated labor may contribute to fatigue, which can delay(link) onset of milk production and can also increase the risk of (link)accidental suffocation of the infant. No mother plans to fall asleep with her baby in the bed, but if parents are awake for 36+ hours, their risks for falling asleep while breastfeeding or holding their baby increases.
Substance use. About 10% of babies in our facility are affected by maternal substance use; about half of these are affected by opioids, whether illicit drugs, prescription drugs, or medication-assisted treatment (MAT) drugs such as methadone and buprenorphine. We can and do support breastfeeding in women who are stable in recovery, even if on MAT, but we recognize that these women may have unique stressors that may make breastfeeding more difficult. Infants who are experiencing withdrawal often have disorganized feeding. Hunger can exacerbate withdrawal, and weight loss is a symptom of withdrawal. These infants do stay in the hospital longer for observation; my threshold to start supplemental feedings is lower since they are at risk for significant weight loss.
Breast anatomy. A history of augmentation or reduction surgery may impact milk production or transfer. Wide-spaced, “tubular” breasts may be an indicator of insufficient glandular tissue. Flat or inverted nipples may present difficulty with latching; a breast shield may help, but the use of a shield should prompt careful follow up of feeding, milk transfer, and weight gain.
Feeding assessment. Every breastfeeding dyad should have an evaluation of feeding by a lactation consultant or clinician with expertise. Latch, nipple pain, and evidence of transfer, such as audible swallowing, are one part of the assessment. Can the mother get the baby on independently or does she require assistance? If the nurse has had to get the baby latched for every feeding, the dyad is not ready for discharge.
Anatomy of the infant’s mouth. Tongue ties and other anatomical considerations may present specific challenges to feeding. (Link) Frenulotomy and lysis of lip ties have become common. Infants who may be at risk for feeding difficulty should be followed very closely, whether or not they have surgical intervention.
Timing of weight assessment. A 7% loss has different implications depending on the day/hour or age. If the weight was done 16 hours earlier on the evening shift before the morning of discharge, I request a repeat weight.
Gestational age. Late preterm (LPT) infants are often cared for in the well-baby setting and may masquerade as healthy term infants, but they are not. LPTs may have excessive weight loss; readmission rates for weight loss, jaundice, and other complications are up to three times higher than for term infants. In our facility, late preterm infants are observed in the hospital setting for a minimum of 72 hours. Our protocol for the care of the LPT follows the recommendations of the Academy of Breastfeeding Medicine: we initiate supplemental feedings for a weight loss of ≥3% by 24 hours or ≥7% by day 3 or, of course, sooner if there is evidence of hypoglycemia, dehydration, jaundice or poor feeding.
Birth weight. We assess weight loss by percentage since babies come in many sizes…however, a 7% weight loss in a baby who weighed five pounds at birth looks different than the same percentage in a large infant who has more reserves of fat and glycogen.
Output. Passage of urine and stool are unreliable indicators of intake, but no or very low output suggests poor intake. A breastfed infant may have only 1-2 wet diapers per 24 hours in the first day or two, but as mother’s milk comes in, the output should increase because of colostrum amounts increase. I always discuss watching output at home and contacting the pediatrician promptly if the infant is not producing urine or dirty diapers.
Experience. Is this a first baby or has the mother successfully breastfed other children? Did she try breastfeeding before and stop? If so, what were the issues?
Exam. A physical exam includes an assessment of hydration status: fontanels, skin turgor, mucous membranes, as well as general well-being, suck, activity level.
So would I discharge a baby with a greater than 7% weight loss and no supplemental feedings? It depends on the complex thought process that goes into discharge planning. Every mother-baby dyad is unique and requires individualized care. An EWL baby can decline rapidly in 24 and It’s important to teach parents about what signs to look for insufficient breastfeeding so that they can safely supplement until they have their next day follow-up pediatrician appointment. Weekends pose particular concerns. Discharging a baby on a Monday with an outpatient appointment the following day is a very different scenario than discharging on a Friday of a holiday weekend with no possibility of follow up until Tuesday. In certain cases where risk factors are present, such as LBW or prematurity, I may order outpatient weight checks for a few weeks. As well, follow up with a lactation consultant can be invaluable for the mother who needs support.
Resources: Boies, E.G., Vaucher, Y.E. & the Academy of Breastfeeding Medicine (2016). ABM Clinical Protocol #10: Breastfeeding the late preterm (34-36 6/7 weeks of gestation) and early term infants (37-38 6/7 weeks of gestation, second revision 2016. Breastfeeding Medicine, 11 (10).Chantry, C.J., Nommsen-Rivers, L.A., Peerson, J.M., Cohen, R.J. & Dewey, K.G. (2011). Excess weight loss in first-born breastfed newborns relates to maternal intrapartum fluid balance. Pediatrics, 127, e171-9.Eltonsy, S., Blinn, A., Sonier, B., DeRoche, S., Mulaja, A., Hynes, W., Barrieau, A. & Belanger, M. (2017). Intrapartum intravenous fluids for caesarian delivery and newborn weight loss: a retrospective cohort study. BMJ Paediatrics Open 2017 (1).
There are many ways you can support the mission of the Fed is Best Foundation. Please consider contributing in the following ways:
Join us in any of the Fed is Best volunteer and advocacy, groups. Click here to join our health care professionals group. We have: FIBF Advocacy Group, Research Group, Volunteer Group, Editing Group, Social Media Group, Legal Group, Marketing Group, Perinatal Mental Health Advocacy Group, Private Infant Feeding Support Group, Global Advocacy Group, and Fundraising Group. Please send an email to Jody@fedisbest.org if you are interested in joining any of our volunteer groups.
If you need infant feeding support, we have a private support group– Join us here.
If you or your baby were harmed from complications of insufficient breastfeeding please send a message to contact@fedisbest.org
Make a donation to the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign theFed is Best Petition at Change.org today, and share it with others.
Share the stories and the message of theFed is Best Foundation through word-of-mouth, by posting on your social media page and by sending our FREE infant feeding educational resources to expectant moms that you know. Share the Fed is Best campaign letterwith everyone you know.
Print out ourletter to obstetric providers and mail them to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
Write your local elected officials about what is happening to newborn babies in hospitals and ask for the legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
Send us your stories. Share with us your successes, your struggles and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
Send us messages of support. We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
Shop at Amazon Smileand Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!
The Fed is Best Foundation has written about countless cases of serious complications caused by poor standards of breastfeeding management established by multiple exclusive breastfeeding advocacy organizations. The primary causes of these poor outcomes are:
the persistent denial of the seriousness of newborn weight loss
the lack of transparency about the consequences of insufficient feeding complications in patient education and health professional training
and the dangerous obsession with exclusivity in breastfeeding.
Exclusive breastfeeding, according to the WHO, means “the infant receives only breast milk. No other liquids or solids are given – not even water – with the exception of oral rehydration solution, or drops/syrups of vitamins, minerals or medicine.” While breastfeeding is a positive thing to support, the obsession with exclusivity in breastfeeding promotion results in approximately 190,000 newborn admissions a year in the U.S. alone, mostly from complications of jaundice and dehydration caused by underfeeding. This article will discuss the actual reason why exclusively breastfed newborns lose weight and why newborn weight loss is not due to IV fluids given to mothers before delivery. This is to address a commonly circulated unsafe recommendation by exclusive breastfeeding advocates and lactation professionals suggesting we increase the AAP recommended maximum weight loss threshold of 7% and to weigh infants at 24 hours, which would likely increase newborn insufficient feeding complications, hospitalizations, and brain injury.
Part 1: Why a Newborn Loses Weight in the First Days
Let’s start the conversation off with why newborns lose weight in the first days of life. Exclusive breastfeeding advocates have hypothesized that infant weight loss is caused by fluid shifts and “diuresis” or elimination of fluid through urination. Diuresis is defined as overproduction of urine caused by excess body fluid, which should be at least 6-8 wet diapers a day, the normal urine production of a hydrated newborn. In fact, exclusively colostrum-fed newborns, only produce 1-2 wet and dirty diapers a day the first 2 days of life, which is lower than the normal number of wet diapers a day for a hydrated newborn. Therefore, weight loss is not in fact caused by fluid loss.
Here are some basic facts about newborn nutrition:
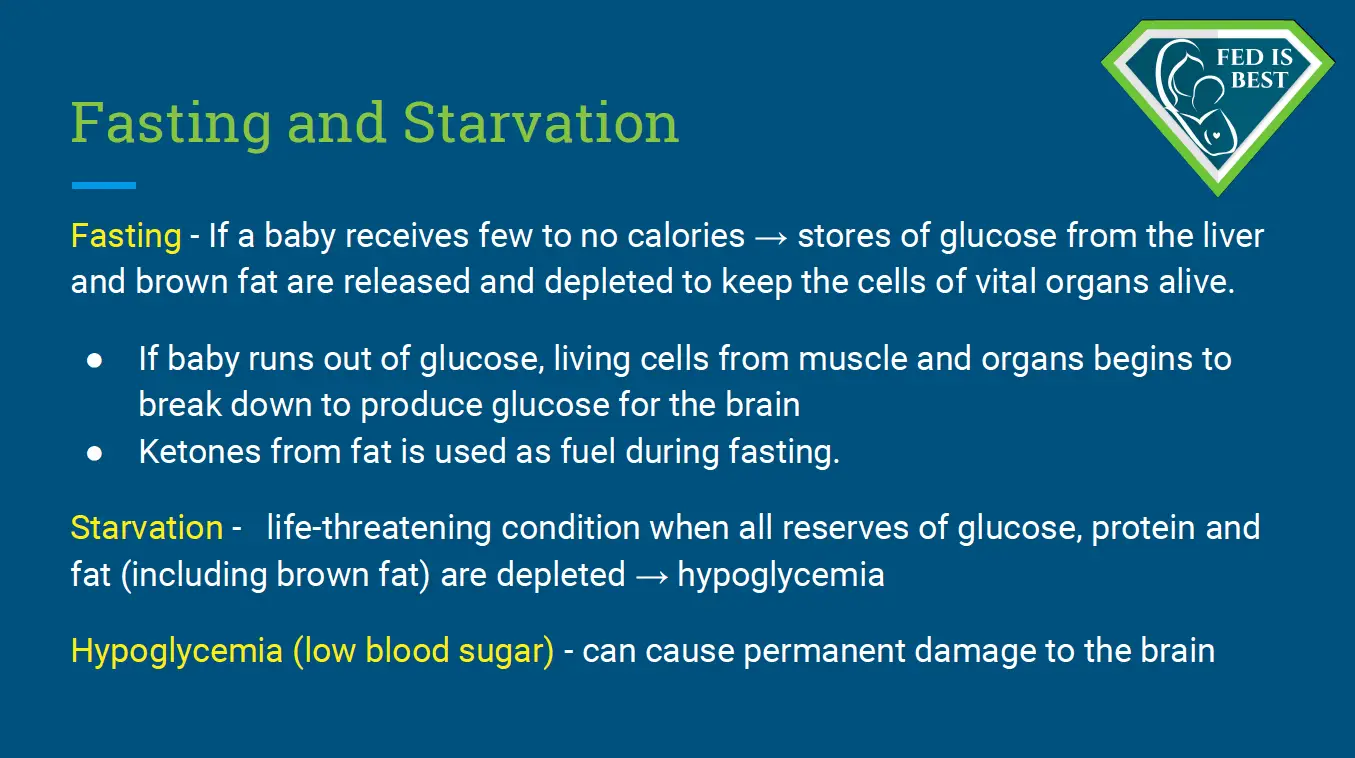
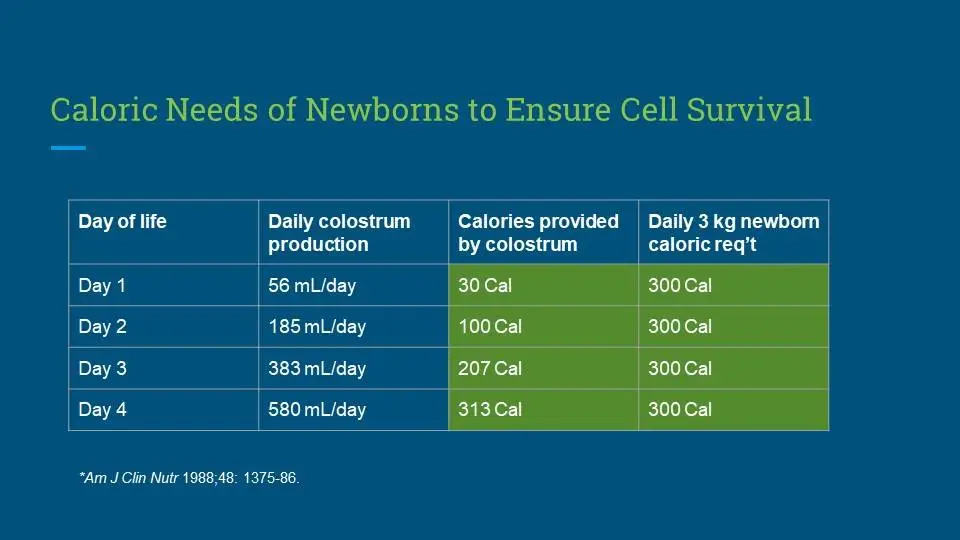
The caloric requirement of a newborn from birth through the first weeks of life is 100-120 Calories/kg/day, a figure that is determined by the number of living cells a baby has to keep alive.
The fluid requirement of a newborn is more variable, which can be affected by how much fluid reserve they are born with. But according to the pediatric literature it is approximately 60-80 mL/kg/day the first 2 days then 100 mL/kg/day thereafter.
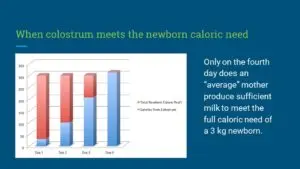
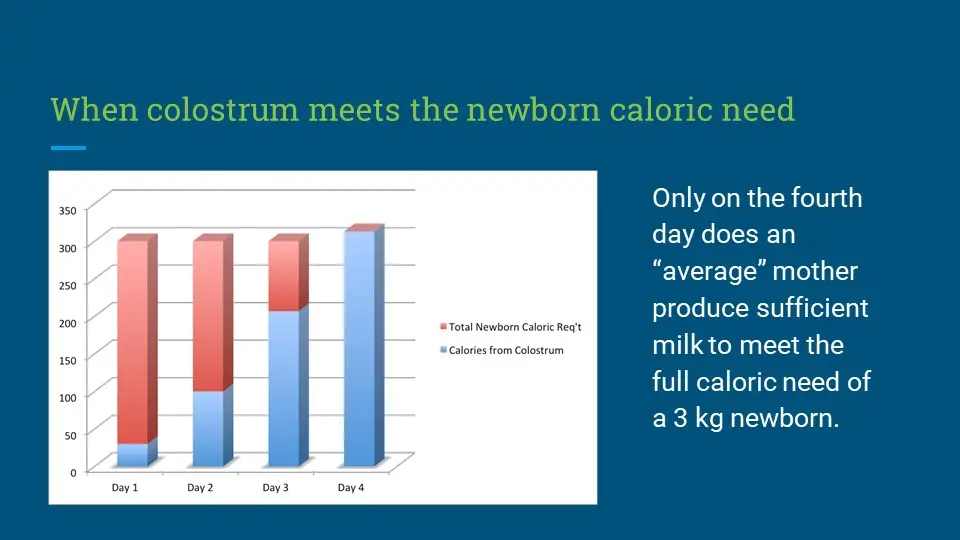
That means a 3 kg newborn needs 300 to 360 Calories per day and 180-240 mL of fluid for the first 2 days and 300 mL thereafter.
6. Does the FIBF believe all exclusively breastfed babies need supplementation before the onset of mature milk?
No, and we never have.
As health care providers, we have an ethical and moral obligation to fully inform mothers of both the benefits and risks of exclusive breastfeeding when promoting exclusive breastfeeding. The high rates of delayed onset of lactogenesis II, as well as conditions that cause a poor transfer of breast milk, carry serious risks to exclusively breastfed newborns, as they depend ondaily increases in calories and fluids until mature milk arrives on day three.
The current research tells us the actual rates of adequate breast milk production are unknown and the current estimates for lactation disruption range from 12-15% or one in eight mothers. We are learning that mothers are experiencing delayed lactogenesis II (onset of full milk supply greater than 72 hours post-birth) commonly, for complex biological and other unknown reasons. However, the fact that something is common does not mean it is normal or ideal.
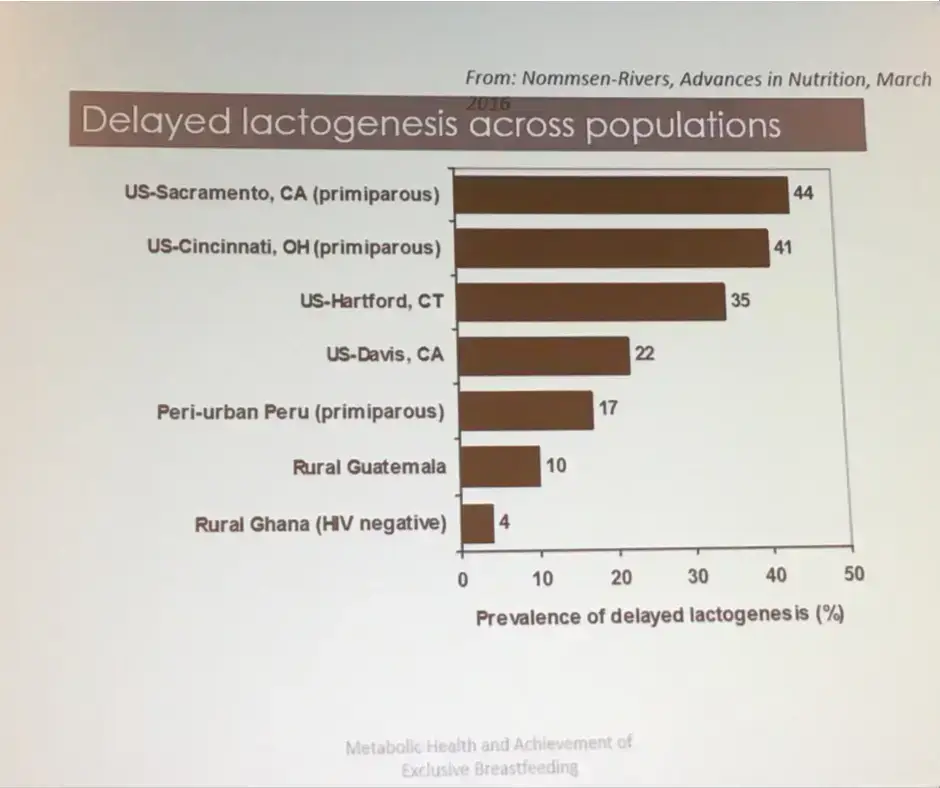
Nommsen-Rivers, Percent of mothers experiencing delayed copious milk production. Presented at 2017 ABM conference
The scientific studies show that delayed onset of lactogenesis II (DOLII), lactation dysfunction and low milk supply (LMS) are common.
Twenty-two percent of mothers experience delayed onset of milk production, which increases the risk of excessive weight loss (>10%) in their newborns seven-fold (Dewey et al., 2003). Delayed onset of lactogenesis II (DOLII) was most common among first-time mothers, mothers with high BMI, and other factors that increased the risk of ineffective breastfeeding.
Delayed onset of lactogenesis II also occurred commonly outside of the U.S. as found in this study from a Brazilian Baby-Friendly Hospital showing it occurred to 19% or almost 1 in 5 mothers. (de Oliveria Rocha et al., 2019)
Another study of first-time mothers showed that an astounding 44% experienced delayed onset of lactogenesis II. (Nommsen-Rivers, et al. 2010). The primary risk factors for DOLII were:
maternal age ≥30 years old
body mass index in the overweight or obese range
birth weight >3600 g
absence of nipple discomfort between 0–3 d postpartum
infant failing to “breastfeed well” ≥2 times in the first 24 h
Colostrum Calories
The scientific literature shows that colostrum, in fact, has fewer calories, containing 54 Calories/100 mL compared to 66-77 Calories/100 mL in mature breast milk (Gidrewicz and Fenton, 2014). Therefore, in the period before lactogenesis II, an exclusively colostrum-fed newborn is “fasting,” meaning that the baby is consuming fewer calories than she is expending, causing weight loss. Babies are dependant on their metabolic reserves until the onset of copious milk production. However, some babies do not have enough reserves and this can result in acute starvation-related complications. These complications can result in irreversible impairments in brain development. The term “starvation” is not intended to be inflammatory; it is a medically accurate diagnosis, the definition of which is explained below.
Complications From Insufficient Breast Milk Research:
Research has shown that among healthy term newborns who are discharged from the hospital, exclusively breastfed newborns are twice as likelyto be readmitted to the hospital, most commonly for hyperbilirubinemia and dehydration. They are also more likely to require more follow-up visits with their pediatricians for concerns related to feeding and adequate weight gain. (Flaherman et al., 2018).
A study from the U.K. showed that among healthy term and near-term newborns, exclusive breastfeeding at discharge doubled the risk for readmission for hypoglycemia (Dassios et al, 2018).
According to a review published in the Journal Of Family Practicein June 2018, “exclusive breastfeeding at discharge from the hospital is likely the single greatest risk factor for hospital readmission in newborns. Term infants who are exclusively breastfed are more likely to be hospitalized compared to formula-fed or mixed-fed infants, due to hyperbilirubinemia, dehydration, hypernatremia, and weight loss.” They estimated that for every 71 infants that are exclusively breastfed, one is hospitalized for serious feeding complications.
Beyond the first days of life, low breast milk production and the inability to produce a full milk supply are common.
Data from the Infant Feeding Practices Study showed that 12% or one in eight women were unable to maintain a breastfeeding relationship for the first year of life. Those most commonly affected were women with high BMIs and women with high depression symptoms (although it is unclear whether the depression is the cause or the effect of failed lactation; Stuebe et al., 2014).
The largest study ever done to measure actual breast milk production was done by Kent et al. in 2016 following 116 breastfeeding mothers with and without breastfeeding problems. The mothers measured all the breast milk they fed their infants over the first month of life through direct feeding (using weighted feeds) and expressed breast milk feeding. This study found that between days 11 and 13, 2/3rd of the mothers could not produce more than the minimum 440 mL required to feed their infant exclusively and between 14 and 28 days, nearly 1/3rd could not produce that minimum. This study likely over-represented mothers will low milk supply given that the study required intensive daily test weighing and logging of pumped milk volumes. However, this is off set by the fact that the investigators defined “low milk supply” as less than 440 mL/day, the amount that is just enough to meet a 2.64 kg or 5.8 lb baby’s daily caloric need (at 110 calories/kg/day). With many babies requiring much more than 440 mL/day at the end of 4 weeks, this aspect of the study underestimated the number of infants who are truly not getting their full requirement and who are likely showing signs of persistent hunger.
Dr. Marianne Neifert, Clinical Professor of Pediatrics at the University of Colorado Denver School of Medicine, co-authored a 1990 study of 319 breastfeeding primiparous (first-time) mothers and found 15% were unable to produce sufficient milk by three weeks after delivery despite intensive lactation support.
In a study of 1065 mothers, 532 or 50% had breastfeeding-related problems. Thirty-one percent affected the mother (e.g., engorgement, fissures, low milk supply, infections, breastfeeding cessation), and 10% affected the newborn (poor suction, neonatal jaundice, pathological weight loss, need for hospital admission). Nine percent affected both the mother and the newborn (Govonni, Richi, 2019). Among the identified risk factors for breastfeeding problems, operative vaginal deliveries and cesarean delivery had the highest associated risk for breastfeeding problems. Other factors like higher maternal age, number of previous deliveries, and lower Apgar scores also increased the risk of DOLII.
Dr. Shannon Kelleher talks about these staggering numbers in her publication, “Biological underpinnings of breastfeeding challenges: the role of genetics, diet, and environment on lactation physiology,” in which she says the prevalence of lactation insufficiency may be much higher, as women internationally cited that their baby was “not satisfied with breast milk” as the primary reasons for weaning prior to 6 months.
Listening to Mothers
The data show that maternal perception of insufficient breast milk and the onset of lactogenesis II is in fact accurate. Listening to the mother instead of encouraging her to distrust her own instincts is critical to helping her reach her breastfeeding goals and maintaining her confidence.
The study called “Maternal Perception of the Onset of Lactation Is a Valid, Public Health Indicator of Lactogenesis Stage II” showed that maternal perception of onset of lactogenesis II (including cases when they are delayed) is valid. Since small volumes of colostrum cannot sustain an infant long-term and prolonged exclusive colostrum feeding can result in complications, maternal perception of onset of copious milk production can be used to determine whether or not an infant’s signs of distress are due to persistent hunger. Infants showing distress before the onset of lactogenesis II are at high risk for feeding complications.
Despite the lack of evidence using the gold-standard of randomized controlled trials (RCTs) showing that supplementation interferes with breastfeeding, health professionals and parents continue to be taught to avoid supplementation until an infant has developed or is at serious risk of insufficient feeding complications. In fact, six RCT studies have shown that in infants with weight loss above the 75th percentile, judicious supplementation with 10 mL (two teaspoons) of donor breast or formula milk after nursing had no effect on long-term breastfeeding, one showing it prevented hospital readmissions in all of the supplemented newborns.
Dr. Flaherman’s research suggests that it is not simply early supplementation that affects breastfeeding outcome, but the volume, delivery mode, and rationale for use that are important. She also suggests that reverse causation may be a factor in breastfeeding cessation in that breastfeeding problems lead to formula use, rather than formula use causing breastfeeding problems. Concerns about limited amounts of formula sensitizing the infant‘s “virgin gut” are speculative and pale in comparison to the risk of brain damage from insufficient food and fluids.
It is unconscionable to scare mothers into withholding supplements while not disclosing the risks of insufficient milk. Would we be even having this conversation if banked donor milk were available for all babies who needed temporary supplementation?
Because of this research, it’s imperative to assess each mother and baby to identify potential individual risk factors for delayed onset of lactogenesis II or low milk supply. This will help the health care team offer timely, temporary supplemental nutrition with banked donor milk or formula milk to prevent complications while providing optimal lactation management and support for identified high-risk dyads. Additionally, the health care team can identify scant or absent colostrum in a high-risk mother through instruction on the manual expression of colostrum.
A comprehensive clinical exam/assessment by the pediatrician, nurse, and lactation consultant care team is necessary every eight hours to evaluate every newborn for safe and adequate intake while breastfeeding, and the mother’s observations should be part of the evaluation. The pediatrician, nurse, LC, and parents should have clearly defined roles in the treatment plan.
The health care team should be evaluating the newborn for:
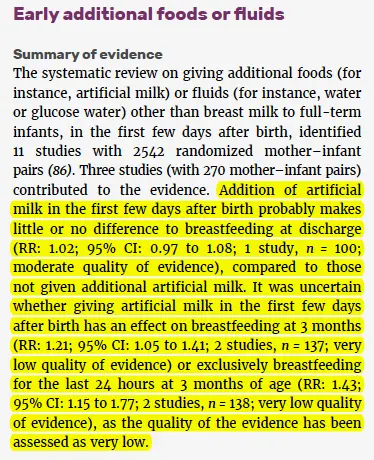
In 2017, the World Health Organization published its guidelines updating its recommendations for“Protecting, Promoting and Supporting Breastfeeding in Facilities Providing Maternity and Newborn Services,”which outlines the evidence for the WHO recommendations on breastfeeding support for newborns in health facilities based on the Ten Steps to Successful Breastfeeding. Here is the evidence presented to justify the recommendation to avoid supplementation in breastfed newborns.
How did the very low quality of evidence turn into moderate-quality evidence for exclusive breastfeeding, particularly when the evidence showed improvement of breastfeeding rates in supplemented breastfed newborns?
7. Do you believe exclusive breastfeeding is a good goal to promote?
We do if a mother wants to exclusively breastfeed and they are fully informed about their individualized risk factors for delayed onset and or potential low milk supply. We promote and educate families about safe exclusive breastfeeding because no other health organization informs parents about the risks of insufficient feeding complications and how easy they are to prevent. To be fully informed, parents must be educated about both the benefits and risks of exclusive breastfeeding. Currently, they are only taught about the benefits and not the risks.
Many mothers want to exclusively breastfeed, and day after day in our support group we help mothers achieve this goal by developing an actionable breastfeeding plan that works for their unique needs. Mothers, especially first-time mothers, have told us that they gave up breastfeeding in the days after birth because they felt that they were not making enough milk, when in fact, their milk arrival was simplydelayed.
If these mothers were educated about their risk factors for delayed onset of milk or insufficient milk supply, how to safely supplement while waiting for their milk to come in, how to increase their milk production, or how to sustain a combo-feeding relationship if their supply is limited, they could go on to have a sustainable breastfeeding relationship instead of losing confidence and stopping breastfeeding altogether.
Our actionable breastfeeding plan provides guidelines for protecting the mother’s milk supply if temporary supplementation is necessary. It’s not true that supplementing decreases the milk supply if a mother’s breasts are adequately stimulated and emptied while supplementing breastfeeding.
Responsiblebreastfeeding education requires families to be taught when to offer safe supplementation of expressed breastmilk or properly prepared formula to protect their baby’s health in the case of insufficient breast milk supply or intake. In some instances, the need for supplementation cannotwait for the consultation with a pediatrician or lactation consultant as doing so may result in serious harm. Many mothers have told us they panicked when they needed to purchase formula and they didn’t know how to safely prepare it or how much to give.
While we do support safe exclusive breastfeeding, we also recognize that some mothers find that it is not working for them or their babies. In those cases, we believe it is important to provide a mother with all of her feeding options, as opposed to encouraging only continued exclusive breastfeeding. Mothers tell us they do not feel heard when there is a clear agenda to support only exclusive breastfeeding. We will support her in her choice, whether that is exclusive breastfeeding, exclusive formula feeding, or a combination. If she states that continued exclusive breastfeeding is important to her, then it is important to us also. We support her feeding goal while prioritizing her infant’s health and safety by recommending supplementation with milk bank donor milk or formula if needed before unsafe conditions occur.
As health care professionals, it is our ethical duty to provide families with all of their options, and exclusive breastfeeding is no exception. We believe the exclusive breastfeeding metric needs immediate reform in light of the current data regarding harm and lack of data showing efficacy. The practice guidelines also need to reflect the need to respects maternal choice. A new alternative to the Baby-Friendly policy is the new Family-Friendly Protocol at Rush Foundation Hospital, whose philosophy is to improve patient outcomes by respecting parental choice to breastfeed, combo-feed or formula feed while providing all the education and support needed to achieve individual feeding goals.
8. If you believe exclusive breastfeeding is an important goal, why are you not promoting it as the ideal or best?
We believe a fully fed baby is the ideal, and for the mothers who are not making enough milk, supplementation with banked donor milk or formula is ideal and best infant feeding. An infant who is exclusively breastfed and is not safely or sufficiently fed is neverideal or best.
When we started our first Facebook page it was titled “Breast is best, if you have enough breast milk.” Mothers started messaging us with their own heartbreaking stories and we’ve taken to heart the thousands of letters we have received from mothers describing the pressure they felt to achieve the “ideal” of exclusive breastfeeding from birth to 6 months, and thefear they have that formula will hurt their babies’ health and future potential. They describe suffering from unbearable shame and guilt when it was not possible for biological, economic, psychological, and/or other personal reasons. Parents told us they desperately needed to hear a more inclusive infant feeding message.The suggestion to change our phraseology from “Breast is best if you have enough breastmilk” to “Fed Is Best” was heard, and this is how #FedIsBest was born. It was the right thing to do.
As the Foundation has grown, we quickly learned that mothers are under the impression that low or delayed milk supply is rare. This puts mothers in a position where they feel they have failedor that they are somehow biologically “abnormal” when they were not producing enough milk, even when they have followed the advice of their lactation professionals. They also feel alone because of how breastfeeding education downplays the prevalence of insufficient milk.
Sadly, mothers have told us they knew their babies were hungry but were taught that feeding their babies formula milk is very harmful when the true harm comes from not feeding their baby enough!Isn’t the first rule in lactation support “feed the baby”? It’s not “push the baby to the limits of his tolerance to avoid a few milliliters of donor milk or formula.”
Parents have unknowingly harmed their infants under the guidance of their lactation educators and health professionals. Some of these mothers lose trust in breastfeeding altogether, which is not what any of us want.
Every lactation consultant knows that if a baby is not getting enough to eat, temporary donor milk or formula supplementation can help breastfeeding, not harm it. Mothers have the right to know and should be empowered with a supplementation plan in case they need it. To do otherwise is to hide the truth and while making mothers dependent on expert help that they may not have access to in the time required to prevent harm.
Having a Plan B does not destroy mothers’ confidence in their bodies; it gives them the confidence to know they can care for their babies no matter what happens, and it gives them the knowledge they need to support their milk supply until the breastfeeding problem can be addressed.
9. Cluster feeding is a well-known phenomenon. Why would you say it’s a sign of the baby not eating enough? The LLL describes the “second-night syndrome” as normal, why do you say it’s not?
Cluster feedingcan be normal when it lasts for a few hours once a day and the baby becomes satisfied after several short feedings. The Academy Of Breastfeeding Medicine defines cluster feeding as “several short feedings close together.” However, mothers are being told constant and prolonged feeding around the clock is “cluster feeding,” and this is where confusion that can result in harm begins. There is a point when cluster feeding becomes a clear sign of insufficient breast milk and/or insufficient transfer of milk, and those signs must be taken seriously for the health and safety of the infant. Mothers tell us they receive conflicting information and as a result, they become very frustrated, lose confidence and want to stop breastfeeding. Or, they persist with exclusive breastfeeding due to incorrect advice, and negative outcomes occur.
It is important to define what cluster feeding really is as health professionals and evaluate and intervene when an infant is in danger of insufficient feeding complications.
There is no stronger maternal drive than to feed your baby and protect him from harm. Mothers experience incredible emotional suffering when they are told their baby “was just cluster feeding,” but it turns out in hindsight they were not eating a sufficient amount, even after nursing for hours. They blame themselves rather than the health professionals who should have taken their concerns seriously.
The “Second Night Syndrome” may be common, but this does not imply that it is normal, safe or ideal. In fact, there has never been a single study documenting the safety of “Second Night Syndrome,” which we know has led to critical illness and injuries in breastfed infants who were not supplemented in a timely or adequate fashion. Our Co-Founder Jody, wrote about the Second Night Syndrome drawing from years of clinical experience working in the Nursery/NICU to inform the article. Some breastfeeding mothers talk about the “Second Night Syndrome” by describing itas absolute hell!They describe their babies as nursing non-stop and as soon as they take baby off the breast they cry frantically. The only time their babies are not crying is when they are breastfeeding. Some mothers say their babies even cry while frantically nursing and nothing consoles them. This is neither safe nor humane to the mother, who is recovering, and the baby who has to endure prolonged hunger. Such conditions not only increase the risk of feeding complications and admissions, but it can also result in accidental bed-sharing and infant falls or suffocation, known as Sudden Unexpected Postnatal Collapse.
The second night of your baby’s life should never be hell. If your baby is crying non-stop despite adequate breastfeeding, an immediate physical assessment by the RN or MD should be made to determine why your baby is crying and if immediate supplementation is necessary.
A check of their glucose, bilirubin, weight and possibly their electrolytes should be performed by a nurse, physician or nurse practitioner to assess whether a newborn is being sufficiently fed and whether supplementation is needed to protect your newborn. Research tells us that 1 in 5 mothers have delayed onset of full milk production, so we simply cannot ignore the abnormal behavior of a non-stop crying baby, knowing there will be babies who need to be supplemented.
Furthermore, the exclusive breastfeeding quality metric has never been proven in randomized, controlled trials to improve breastfeeding rates, while decades of evidence have shown that rigid insistence on this metric increases the risk of harm.
THANK YOU FOR YOUR INTEREST IN THE FED IS BEST FOUNDATION!
Our mission statement is:
The Fed is Best Foundation works to identify critical gaps in current breastfeeding protocols, guidelines, and education programs. We provide families and health professionals with the most up-to-date scientific research, education, and resources to practice safe infant feeding with breast milk, formula, or a combination of both. To be fully informed, parents must be taught about the risks of insufficient breast milk intake while supporting exclusive breastfeeding in order to eliminate preventable hospitalizations for insufficient feeding complications. Finally, we strive to eliminate infant feeding shaming while prioritizing perinatal mental health.
HOW YOU CAN SUPPORT FED IS BEST
There are many ways you can support the mission of the Fed is Best Foundation. Please consider contributing in the following ways:
Join us in any of the Fed is Best volunteer and advocacy, groups. We currently have– Health Care Professional Advocacy Group, Advocacy Group, Research Group, Volunteer Group, Editing Group, Social Media Group, Legal Group, Marketing Group, Maternal Mental Health Advocacy Group, Private Infant Feeding Support Group, Global Advocacy Group, and Fundraising Group. Please send an email to Jody@fedisbest.org– if you are interested in joining any of our volunteer groups. For our health professional advocacy group, join us here.
If you need infant feeding and parenting support, we have a support group– Join us here.
Make a donation to the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign theFed is Best Petition at Change.org today, and share it with others.
Share the stories and the message of theFed is Best Foundation through word-of-mouth, by posting on your social media page and by sending our FREE infant feeding educational resources to expectant moms that you know. Share the Fed is Best campaign letterwith everyone you know.
Print out ourletter to obstetric providers and mail them to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
Write your local elected officials about what is happening to newborn babies in hospitals and ask for legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
Send us your stories. Share with us your successes, your struggles and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
Send us messages of support. We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
Shop at Amazon Smileand Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!