
By Alex Fischer, PhD Candidate, Brooke Orosz, PhD, Jody Segrave-Daly, RN, IBCLC, Lynnette Hafken, MA, IBCLC and Christie Del Castillo-Hegyi, M.D.
Any good magician will tell you that the secret to their trade is misdirection—making the audience look one way while doing something the other way. And even knowing this, most of us are still baffled by a magician’s tricks. So it’s no wonder that Baby-Friendly USA (BFUSA) has tried to employ that same tactic in their statement titled “Fact vs FIB: The Impact of Baby-Friendly on Breastfeeding Initiation Rates.” In this statement written by an anonymous author representing BFUSA, they attempt to dispute the findings of a recent study published in Journal of Pediatrics, “Outcomes from the Centers for Disease Control and Prevention 2018 Breastfeeding Report Card: Public Policy Implications” by Bass et al. This study examines the impact of statewide breastfeeding initiation rates as well as the impact of BFHI facilities on continued breastfeeding after hospital discharge (exclusive or combination). The Fed is Best Foundation read this study and agreed: “Baby-Friendly does not work.” These five words are the instigators of the entire statement by BFUSA and its misrepresentation of a very robust scientific study.
The anonymous author attempts to point out flaws in the methodology of the Bass et al. paper referenced above citing what they believe are errors by the study authors that led to incorrect conclusions. They offer their own analysis of the data showing that nationwide “ever breastfed” rates increased with increasing births at BFHI hospitals over time. However, the BFHI’s purpose isn’t just to increase “ever breastfed” rates, which can include mothers who tried to breastfeed even once in the hospital, but to promote continued breastfeeding after discharge (Step 5 of the Ten Steps). The BFUSA statement claims that the “…authors selected data from the CDC’s Breastfeeding Report Card from only two years. They took the state-by-state ‘Percent of live births occurring at Baby-Friendly Facilities’ data from 2018 and compared these to the state-by-state ‘Ever Breastfed’ data from 2015,” suggesting they should have looked at the data as early as 2007. In fact, the study actually gives the BFHI the benefit of the doubt by only examining its best years, ignoring earlier years when the percent of BFHI births were less than 5%. Even at its peak, BFHI does not correlate with increased continued breastfeeding, exclusive or otherwise. This, remember, is their goal.

Figure 1 from Bass et al, J Pediatrics, 2019 shows increase in breastfeeding with breastfeeding initiation and no effect related to the percent of births occurring at BFHI hospitals
What did the study find? With higher statewide breastfeeding initiation rates, we see an increase in sustained breastfeeding. Higher breastfeeding initiation not only reflects baseline interest among mothers to breastfeed but also the strength of healthcare facilities within the state to effectively teach mothers how to breastfeed. Also, without initiating breastfeeding, one cannot continue to do it exclusively or otherwise. However, was the increase in breastfeeding initiation and continued breastfeeding due to the BFHI? If the BFHI contributed to higher continued breastfeeding rates, then states with more births at BFHI hospitals should have higher sustained breastfeeding rates. Did it? That answer is a resounding NO. The authors plotted percent of BFHI hospital births to statewide rates of exclusive breastfeeding at 3 and 6 months (Figure 2), any breastfeeding at 6 and 12 months (Figure 1) and breastfeeding initiation (Figure 3), the very job they are enlisted to help hospitals achieve, and found no effect on either breastfeeding initiation rates or continued breastfeeding.

Figure 2. Exclusive Breastfeeding at 3 and 6 months increases with increased statewide breastfeeding initiation rates and but not with higher rates of BFHI births
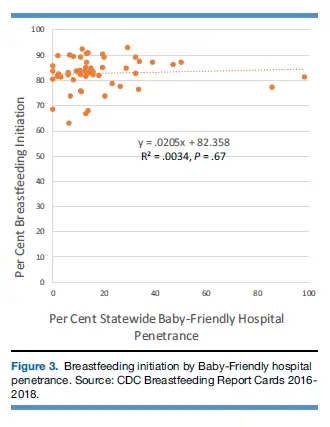
Figure 3 shows higher rates of BFHI births had no effect on breastfeeding initiation rates. The two states with >80% BFHI births actually scored lower than the majority of states with less than 40% BFHI births.
BFUSA’s argument is that they should have looked at national trends in “ever breastfeeding,” not statewide figures. BFUSA claims “…that the authors committed an error known to statisticians as an ecological fallacy by comparing states, instead of comparing data across the whole country. They did not account for the fact that states have vastly different baseline breastfeeding rates due to underlying socio-demographics.” However, one cannot separate from national data the influence of the BFHI hospital program from the general rise in breastfeeding rates since 1970 and again since 1990 when the WHO recommended exclusive breastfeeding from birth to 6 months.

Breastfeeding Initiation Rates vs. % Live Births in BFHI Facilities shows an 8% increase between 2007 and 2015…however
Breastfeeding Initiation has been increasing about 1.4% every year between 1990-2007 (Wright and Schanler, Journal of Nutrition, 2001). At this rate, an increase of 11% would be expected over the 8 years between 2007 and 2015 on BFUSA’s graph.
The only way to measure the influence of the BFHI itself would be to look at differences in statewide rates of continued breastfeeding to see if states with a higher proportion of births at BFHI hospitals performed better. While BFUSA claims the study didn’t account for different baseline state breastfeeding rates, the study, in fact, did exactly that when they measured individual states’ continued breastfeeding and breastfeeding initiation rates. That is how they discovered that higher initiation has more to do with higher continued breastfeeding rates, thus teasing out the effects of BFHI certification from this baseline phenomenon.
So what do they mean by ecological fallacy? First, we need to examine what an ecological fallacy is. It is defined as making conclusions about an individual based on data obtained from a group. To remedy to this fallacy, the author of the BFUSA statement claims that only nationwide data should be examined, not individual state data. However, that would indeed be drawing individual conclusions from an even larger group of data, which is the very definition of ecological fallacy. They attempted to make us look the other way by introducing an impressive sounding term that most people don’t know and make it look like the study authors made an error. In fact, they are asking us to commit an even worse error by relying on national data instead of state data, which worsens the ecological fallacy. It’s ironic that they would argue that ecological fallacy makes the Bass study unreliable when the entire premise of exclusive breastfeeding promotion relies on ecological fallacy. All the listed benefits of exclusive breastfeeding relies on the belief that even slight advantages found in breastfed babies when averaged across the population must apply to every baby. In reality, some babies are adequately fed and protected by exclusive breastfeeding, but some babies are harmed if they don’t receive enough.
But to take a step back, if you look at overall breastfeeding initiation rates, yes, the rates are increasing— by 9.4% of the population over 11 years (2004-2015 CDC Breastfeeding Report Data). And to be robust, we have to ask:
At what cost?
What was the cost of the rise of mothers encouraged to pursue exclusive breastfeeding from birth without adequate education on the risks of following the BFHI policy? We can point to the staggering statistics of 1 in 71 to 1 in 25 babies being readmitted due to dehydration and jaundice, both complications of underfeeding. Then there are the :
- 10% of exclusively breastfed newborns who develop hypoglycemia,
- 12-25% who develop excessive jaundice,
- and the previously unrecognized 36% who develop hypernatremia.
All these conditions are known causes of newborn brain injury, long-term disability and increased risk of death.
Not to mention mothers who suffer as they are
- pressured to exclusively breastfeed even if their infants are showing hours to days of persistent hunger,
- shamed into caring for their infants 24 hours a day despite exhaustion immediately after childbirth,
- forced to suffer inhumane levels of sleep deprivation that put their infants at risk of suffocation and falls from accidental bed-sharing,
- lied to about the risks of formula, the size of their child’s stomach, the nutritional content of colostrum, the prevalence of low milk production and the signs and consequences of persistent infant hunger,
- not listened to when they say their babies are hungry,
- and forced to watch their infants suffer serious insufficient feeding complications that require hospital treatment and may negatively impact them for the rest of their lives.
The worst part is that they suffer these discomforts and negative outcomes while complying with Baby-Friendly rules that have been shown to have little to no effect on continued breastfeeding rates after discharge, as evidenced by this paper and by the WHO’s own 2017 breastfeeding guidelines, which we discuss in this article.
BFHI is a dangerous and broken system with no data documenting safety, decades of evidence documenting harm, and ultimately, it isn’t “friendly” to babies or mothers (though to be fair, they never claimed to be mother-friendly anyway).
State-specific breastfeeding data help us understand what states are performing better or worse and whether the BFHI hospital credential has anything to do with it. The study clearly shows that BFHI credentialing had no effect on either breastfeeding initiation or continued breastfeeding. Of course, such data would threaten the very existence of BFUSA, therefore attempts to discredit it are expected. If they are willing to routinely hide evidence of the risks of their protocol from families, they are willing to hide evidence of their lack of efficacy. Clearly the issue that BFUSA takes with the presentation of the data has far more to do with the conclusions that they want to draw rather than any severe methodological flaws. True to form, they don’t even attempt to counter our accounting of the risks of the BFHI policy, because they can’t; those harms have been repeatedly documented and are uncontested. When you are up against a wall and a well-done study clearly shows your program is ineffective while others provide abundant evidence of serious and irreversible harm, the only weapon you have left is misdirection.
BFUSA and the WHO continues to claim that over 820,000 lives and 300 billion USD can be saved globally by getting almost all mothers to exclusively breastfeed (a claim that has never been verified with real data). When approximately 15% of mothers have persistent milk insufficiency in the first 3 weeks, when 22–44% have delayed copious milk production and a still unmeasured percent cannot physically produce their infants’ full daily nutritional requirement through the first 6 months even with intensive lactation support, what is the cost of the hundreds of thousands of extended and repeat admissions a year that would occur in the U.S. alone and millions globally for hyperbilirubinemia, dehydration, hypoglycemia and failure to thrive? What are the costs of the long-term neurological and health consequences related to infant starvation caused by the BFHI? It costs a hospital thousands of dollars to become BFHI certified; that money could be used for more effective—and safer—breastfeeding support. That support should recognize that a significant portion of mothers and babies cannot exclusively breastfeed safely, and that for those infants, timely and adequate supplementation is imperative to prevent serious long-term health consequences.
So we urge you to not be distracted by BFUSA’s attempt to take credit for the general rise in breastfeeding that has been occurring since the 1970s even without their influence, and instead focus on the terrible consequences of the BFHI. Never has there been a policy so reviled by both medically-trained health professionals and patients alike that provides so little benefit while increasing the risks of brain injury and death to infants than the BFHI. BFUSA is using a classic misdirection, and we cannot let them use smoke and mirrors to trick the public into ignoring the harm they have caused.
References
Bass, Joel L., Tina Gartley, and Ronald Kleinman. 2019. “Outcomes from the Centers for Disease Control and Prevention 2018 Breastfeeding Report Card: Public Policy Implications.” The Journal of Pediatrics, October. https://doi.org/10.1016/j.jpeds.2019.08.059.
Wright, A., and R. Schanler. 2001. “The Resurgence of Breastfeeding at the End of the Second Millennium.” The Journal of Nutrition 131 (2): 421S-5S. https://doi.org/10.1093/jn/131.2.421S.
Wilson, Joseph L., and Bridgid H. Wilson. 2018. “Is the ‘Breast Is Best’ Mantra an Oversimplification?” The Journal of Family Practice 67 (6): E1–9.
Flaherman, Valerie, Eric W. Schaefer, Michael W. Kuzniewicz, Sherian X. Li, Eileen M. Walsh, and Ian M. Paul. 2017. “Health Care Utilization in the First Month After Birth and Its Relationship to Newborn Weight Loss and Method of Feeding.” Academic Pediatrics, December. https://doi.org/10.1016/j.acap.2017.11.005.
Tarcan, Aylin, Filiz Tiker, Nilgün Salk Vatandaş, Ayşegül Haberal, and Berkan Gürakan. 2005. “Weight Loss and Hypernatremia in Breast-Fed Babies: Frequency in Neonates with Non-Hemolytic Jaundice.” Journal of Paediatrics and Child Health 41 (9–10): 484–87. https://doi.org/10.1111/j.1440-1754.2005.00688.x.
Information for Hospitals: Ensuring Safety for Breastfed Newborns
U.S. Study Shows Baby-Friendly Hospital Initiative Does Not Work
CONTACT US/VOLUNTEER
THANK YOU FOR YOUR INTEREST IN THE FED IS BEST FOUNDATION!
Our mission statement is:
The Fed Is Best Foundation works to identify critical gaps in the current breastfeeding protocols, guidelines, and education programs and provides families and health professionals with the most up-to-date scientific research, education, and resources to practice safe infant feeding, with breast milk, formula or a combination of both.
Above all, we strive to eliminate infant feeding shaming and eliminate preventable hospitalizations for insufficient feeding complications while prioritizing perinatal mental health.
HOW YOU CAN SUPPORT FED IS BEST
There are many ways you can support the mission of the Fed is Best Foundation. Please consider contributing in the following ways:
- Join us in any of the Fed is Best volunteer and advocacy, groups. Click here to join our health care professionals group. We have: FIBF Advocacy Group, Research Group, Volunteer Group, Editing Group, Social Media Group, Legal Group, Marketing Group, Perinatal Mental Health Advocacy Group, Private Infant Feeding Support Group, Global Advocacy Group, and Fundraising Group. Please send an email to Jody@fedisbest.org if you are interested in joining any of our volunteer groups.
- If you need infant feeding support, we have a private support group– Join us here.
- If you or your baby were harmed from complications of insufficient breastfeeding please send a message to contact@fedisbest.org
- Make a donation to the Fed is Best Foundation. We are using funds from donations to cover the cost of our website, our social media ads, our printing and mailing costs to reach health providers and hospitals. We do not accept donations from breast- or formula-feeding companies and 100% of your donations go toward these operational costs. All the work of the Foundation is achieved via the pro bono and volunteer work of its supporters.
- Sign our petition! Help us reach our policymakers, and drive change at a global level. Help us stand up for the lives of millions of infants who deserve a fighting chance. Sign the Fed is Best Petition at Change.org today, and share it with others.
- Share the stories and the message of the Fed is Best Foundation through word-of-mouth, by posting on your social media page and by sending our FREE infant feeding educational resources to expectant moms that you know. Share the Fed is Best campaign letter with everyone you know.
- Write a letter to your health providers and hospitals about the Fed is Best Foundation. Write to them about feeding complications your child may have experienced.
- Print out our letter to obstetric providers and mail them to your local obstetricians, midwives, family practitioners who provide obstetric care and hospitals.
- Write your local elected officials about what is happening to newborn babies in hospitals and ask for the legal protection of newborn babies from underfeeding and of mother’s rights to honest informed consent on the risks of insufficient feeding of breastfed babies.
- Send us your stories. Share with us your successes, your struggles and everything in between. Every story saves another child from experiencing the same and teaches another mom how to safely feed her baby. Every voice contributes to change.
- Send us messages of support. We work every single day to make infant feeding safe and supportive of every mother and child. Your messages of support keep us all going.
- Shop at Amazon Smile and Amazon donates to Fed Is Best Foundation.
Or simply send us a message to find out how you can help make a difference with new ideas!
For any urgent messages or questions about infant feeding, please do not leave a message on this page as it will not get to us immediately. Instead, please email christie@fedisbest.org.
Thank you and we look forward to hearing from you!

One thought on “Baby-Friendly: Failure and the Art of Misdirection”